Devon L Mitchell, John Pearce, Patrick King, Sepehr Sani
{"title":"Rubrospinal activation during asleep subthalamic nucleus deep brain stimulation: a false localizing sign. Illustrative case.","authors":"Devon L Mitchell, John Pearce, Patrick King, Sepehr Sani","doi":"10.3171/CASE23100","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Deep brain stimulation (DBS) can be a life-changing intervention for patients with Parkinson's disease (PD), but its success is largely dependent on precise lead placement. The subthalamic nucleus (STN) is one of the most common surgical targets of DBS, but the close anatomical and physiological resemblance of the STN to the mediocaudal red nucleus renders these landmarks difficult to distinguish.</p><p><strong>Observations: </strong>We present an atypical case in which targeted localization of the STN resulted in symptoms pathognomonic of rubrospinal tract (RST) stimulation. A 79-year-old female with a 12-year history of right-hand resting tremor due to medically refractory PD presented for asleep bilateral STN-DBS surgery. Right STN intraoperative testing revealed left hand and elbow flexion contractures, initially suggestive of corticospinal tract activation, despite imaging studies demonstrating reasonable lead placement in the central dorsolateral STN. The lead was moved anteromedially near the medial border of the STN, but stimulation at this location revealed similar but more robust flexor hand and arm contractures, without any extraocular muscle involvement. Thus, activation of the RST was suspected.</p><p><strong>Lessons: </strong>Isolated activation of the RST is possible during STN-DBS surgery. Its identification can help avoid false localization and suboptimal lead placement.</p>","PeriodicalId":16554,"journal":{"name":"Journal of Neurosurgery: Case Lessons","volume":"6 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9c/3f/CASE23100.PMC10555643.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurosurgery: Case Lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE23100","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Deep brain stimulation (DBS) can be a life-changing intervention for patients with Parkinson's disease (PD), but its success is largely dependent on precise lead placement. The subthalamic nucleus (STN) is one of the most common surgical targets of DBS, but the close anatomical and physiological resemblance of the STN to the mediocaudal red nucleus renders these landmarks difficult to distinguish.
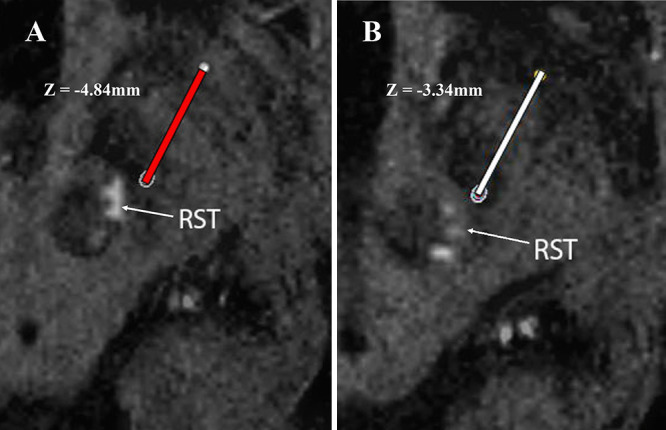
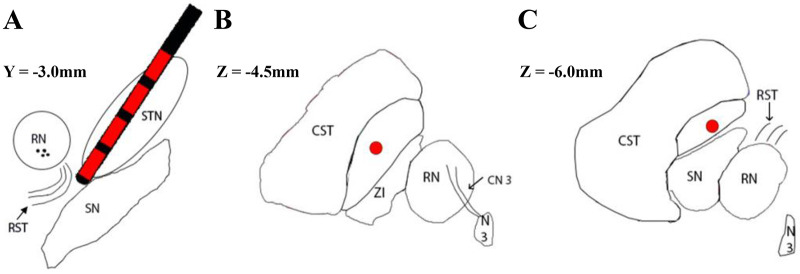
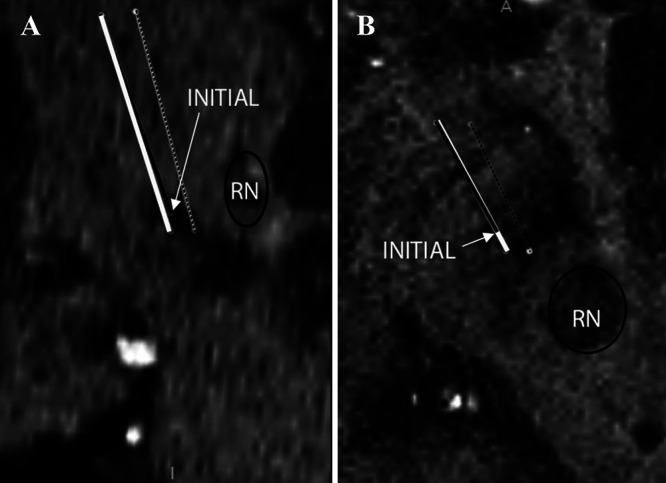
Observations: We present an atypical case in which targeted localization of the STN resulted in symptoms pathognomonic of rubrospinal tract (RST) stimulation. A 79-year-old female with a 12-year history of right-hand resting tremor due to medically refractory PD presented for asleep bilateral STN-DBS surgery. Right STN intraoperative testing revealed left hand and elbow flexion contractures, initially suggestive of corticospinal tract activation, despite imaging studies demonstrating reasonable lead placement in the central dorsolateral STN. The lead was moved anteromedially near the medial border of the STN, but stimulation at this location revealed similar but more robust flexor hand and arm contractures, without any extraocular muscle involvement. Thus, activation of the RST was suspected.
Lessons: Isolated activation of the RST is possible during STN-DBS surgery. Its identification can help avoid false localization and suboptimal lead placement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


