Lindsey A. Wallace DScPAS, PA-C , Kelsey K. Schuder CNP, MSN, MPH , Vicki Loeslie DNP , Andrew C. Hanson MS , Clifford Ongubo DNP , Elaine Chiarelly CNP, MSN , Gregory Schalla PA-C , Kathleen Hinson Meek PA-C , Donald Springer CNP
{"title":"Improving Communication in the Medical Intensive Care Unit Through Standardization of Handoff Format: A Quality Improvement Project","authors":"Lindsey A. Wallace DScPAS, PA-C , Kelsey K. Schuder CNP, MSN, MPH , Vicki Loeslie DNP , Andrew C. Hanson MS , Clifford Ongubo DNP , Elaine Chiarelly CNP, MSN , Gregory Schalla PA-C , Kathleen Hinson Meek PA-C , Donald Springer CNP","doi":"10.1016/j.mayocpiqo.2023.05.006","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>To decrease interruptions in handoff, increase compliance with a structured verbal handoff format, and increase compliance with handoff template completion in electronic medical records without increasing the length of handoff time.</p></div><div><h3>Patients and Methods</h3><p>The project timeline was from April 1, 2019, to February 1, 2020. Define phase data were obtained through a survey of stakeholders to identify the gap in needs. The baseline data included components from the illness severity, patient summary, action list, situational awareness and contingency plans, and synthesis by receiver (IPASS) handoff tool because this tool best aligned with information identified in the define phase. Observational data were collected in person and reviewed via audio recording for accuracy. Results were analyzed to determine adherence to the chosen intervention, the IPASS handoff tool, on which the stakeholders were educated and assessed prior to implementation. Five plan-do-study-act cycles were completed over 3 months to optimize the intervention. Final data were collected and analyzed using the same method as baseline data.</p></div><div><h3>Results</h3><p>After implementation of the IPASS handoff tool, there were more care plan components mentioned in the provider handoffs across all unique IPASS components, there were fewer observed distracting events, and there was increased compliance with electronic medical record handoff completion. The time of handover increased by 3 minutes.</p></div><div><h3>Conclusion</h3><p>A standardized handoff tool improved communication during provider handoffs by increasing the mention of pertinent details and reducing distracting events during handoff.</p></div>","PeriodicalId":94132,"journal":{"name":"Mayo Clinic proceedings. Innovations, quality & outcomes","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/da/d7/main.PMC10345749.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mayo Clinic proceedings. Innovations, quality & outcomes","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2542454823000358","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
To decrease interruptions in handoff, increase compliance with a structured verbal handoff format, and increase compliance with handoff template completion in electronic medical records without increasing the length of handoff time.
Patients and Methods
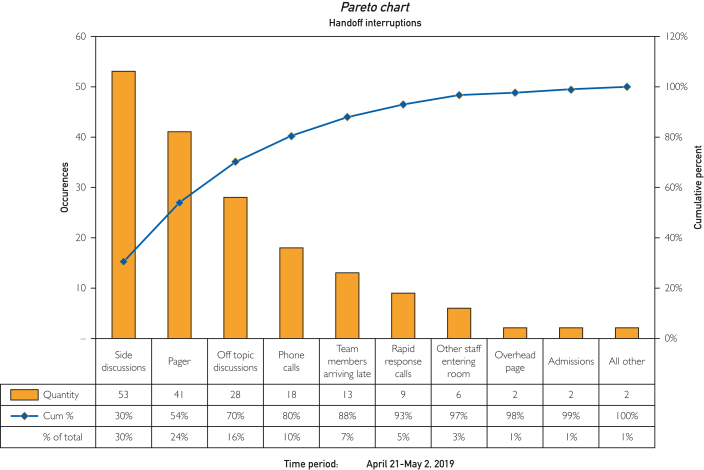
The project timeline was from April 1, 2019, to February 1, 2020. Define phase data were obtained through a survey of stakeholders to identify the gap in needs. The baseline data included components from the illness severity, patient summary, action list, situational awareness and contingency plans, and synthesis by receiver (IPASS) handoff tool because this tool best aligned with information identified in the define phase. Observational data were collected in person and reviewed via audio recording for accuracy. Results were analyzed to determine adherence to the chosen intervention, the IPASS handoff tool, on which the stakeholders were educated and assessed prior to implementation. Five plan-do-study-act cycles were completed over 3 months to optimize the intervention. Final data were collected and analyzed using the same method as baseline data.
Results
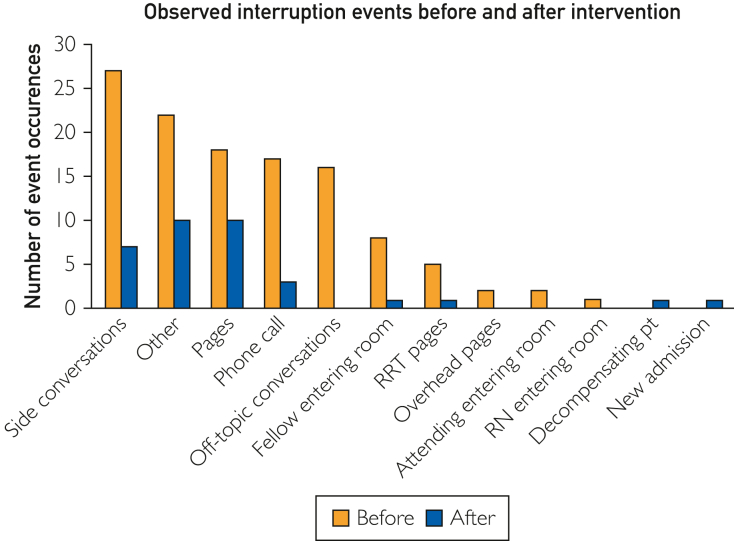
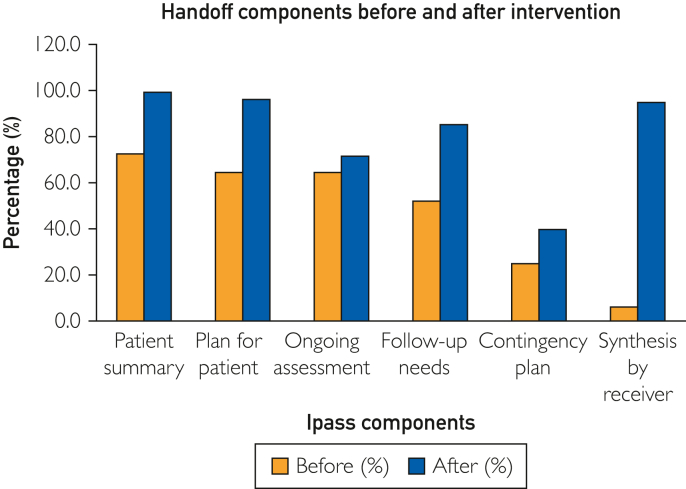
After implementation of the IPASS handoff tool, there were more care plan components mentioned in the provider handoffs across all unique IPASS components, there were fewer observed distracting events, and there was increased compliance with electronic medical record handoff completion. The time of handover increased by 3 minutes.
Conclusion
A standardized handoff tool improved communication during provider handoffs by increasing the mention of pertinent details and reducing distracting events during handoff.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


