{"title":"Anti-N-methyl D-aspartate receptor encephalitis presenting with the new-onset refractory status epilepticus.","authors":"Murat Alemdar, Turkan Acar, Sule Dalkilic","doi":"10.14744/nci.2021.70431","DOIUrl":null,"url":null,"abstract":"<p><p>New-onset refractory status epilepticus (NORSE) is a rare entity referring refractory status epilepticus (SE) in a patient without a history of epilepsy or an apparent cause. Herein, we report on a 31-year-old young female of anti-N-methyl D-aspartate (NMDA) receptor encephalitis admitted with NORSE. Her complaints began a week ago with a fever, meaningless movements, restlessness, and talking to herself. She had a history of operation for ovarian teratoma 10 years ago. Electrocardiography, hemogram, biochemistry, and neuroimaging were normal. Due to recurrent seizures despite intravenous diazepam infusions, phenytoin infusion was introduced, reducing the duration and frequency of seizures. Electroencephalogram (EEG) revealed a generalized slow background activity with low voltage and delta waves in left hemisphere derivatives without any epileptiform discharge. Autoimmune encephalitis panel revealed a positive anti-NMDAR receptor antibody. Intravenous immunoglobulins were given for 5 days. She was improved clinically and did not have a recurrent seizure. The history of our case emphasizes the importance of EEG and CSF antibody tests to reach the underlying etiology in patients presenting with refractory SE and neuropsychiatric symptoms of an unknown cause. Application of a proper treatment promptly with this approach could prevent the potential morbidity and mortality in these patients.</p>","PeriodicalId":19164,"journal":{"name":"Northern Clinics of Istanbul","volume":"10 3","pages":"385-389"},"PeriodicalIF":0.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a3/07/NCI-10-385.PMC10331237.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Northern Clinics of Istanbul","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/nci.2021.70431","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 1
Abstract
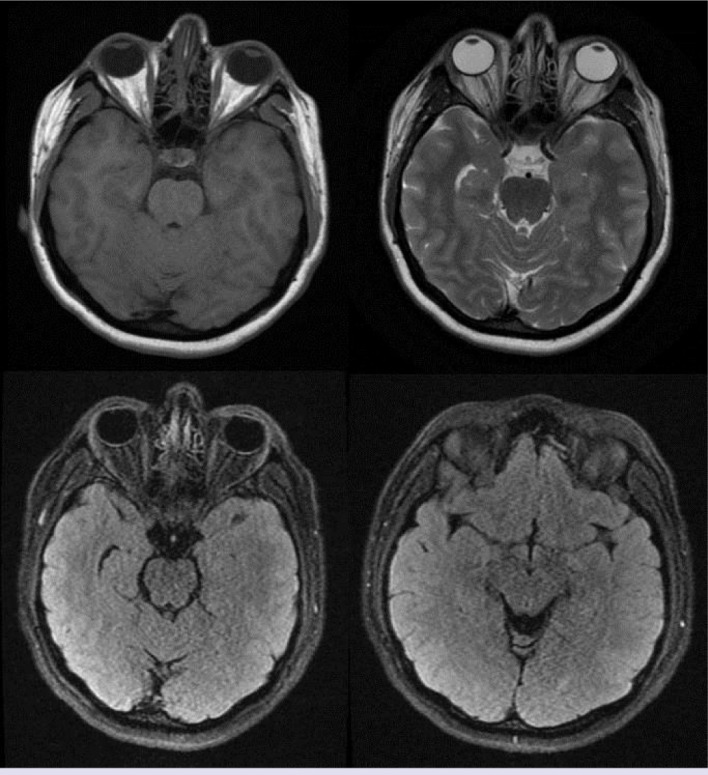
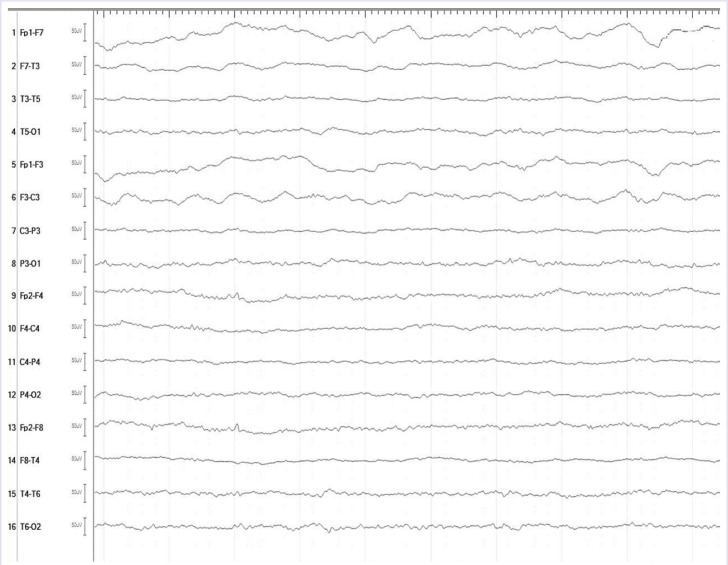
New-onset refractory status epilepticus (NORSE) is a rare entity referring refractory status epilepticus (SE) in a patient without a history of epilepsy or an apparent cause. Herein, we report on a 31-year-old young female of anti-N-methyl D-aspartate (NMDA) receptor encephalitis admitted with NORSE. Her complaints began a week ago with a fever, meaningless movements, restlessness, and talking to herself. She had a history of operation for ovarian teratoma 10 years ago. Electrocardiography, hemogram, biochemistry, and neuroimaging were normal. Due to recurrent seizures despite intravenous diazepam infusions, phenytoin infusion was introduced, reducing the duration and frequency of seizures. Electroencephalogram (EEG) revealed a generalized slow background activity with low voltage and delta waves in left hemisphere derivatives without any epileptiform discharge. Autoimmune encephalitis panel revealed a positive anti-NMDAR receptor antibody. Intravenous immunoglobulins were given for 5 days. She was improved clinically and did not have a recurrent seizure. The history of our case emphasizes the importance of EEG and CSF antibody tests to reach the underlying etiology in patients presenting with refractory SE and neuropsychiatric symptoms of an unknown cause. Application of a proper treatment promptly with this approach could prevent the potential morbidity and mortality in these patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


