Imran Noorani, Kastytis Sidlauskas, Sean Pellow, Reece Savage, Jeannette L Norman, David S Chatelet, Mark Fabian, Paul Grundy, Jeng Ching, James A R Nicoll, Delphine Boche
{"title":"Clinical impact of anti-inflammatory microglia and macrophage phenotypes at glioblastoma margins.","authors":"Imran Noorani, Kastytis Sidlauskas, Sean Pellow, Reece Savage, Jeannette L Norman, David S Chatelet, Mark Fabian, Paul Grundy, Jeng Ching, James A R Nicoll, Delphine Boche","doi":"10.1093/braincomms/fcad176","DOIUrl":null,"url":null,"abstract":"<p><p>Glioblastoma is a devastating brain cancer for which effective treatments are required. Tumour-associated microglia and macrophages promote glioblastoma growth in an immune-suppressed microenvironment. Most recurrences occur at the invasive margin of the surrounding brain, yet the relationships between microglia/macrophage phenotypes, T cells and programmed death-ligand 1 (an immune checkpoint) across human glioblastoma regions are understudied. In this study, we performed a quantitative immunohistochemical analysis of 15 markers of microglia/macrophage phenotypes (including anti-inflammatory markers triggering receptor expressed on myeloid cells 2 and CD163, and the low-affinity-activating receptor CD32a), T cells, natural killer cells and programmed death-ligand 1, in 59 human <i>IDH1</i>-wild-type glioblastoma multi-regional samples (<i>n</i> = 177; 1 sample at tumour core, 2 samples at the margins: the infiltrating zone and leading edge). Assessment was made for the prognostic value of markers; the results were validated in an independent cohort. Microglia/macrophage motility and activation (Iba1, CD68), programmed death-ligand 1 and CD4<sup>+</sup> T cells were reduced, and homeostatic microglia (P2RY12) were increased in the invasive margins compared with the tumour core. There were significant positive correlations between microglia/macrophage markers CD68 (phagocytic)/triggering receptor expressed on myeloid cells 2 (anti-inflammatory) and CD8<sup>+</sup> T cells in the invasive margins but not in the tumour core (<i>P</i> < 0.01). Programmed death-ligand 1 expression was associated with microglia/macrophage markers (including anti-inflammatory) CD68, CD163, CD32a and triggering receptor expressed on myeloid cells 2, only in the leading edge of glioblastomas (<i>P</i> < 0.01). Similarly, there was a positive correlation between programmed death-ligand 1 expression and CD8<sup>+</sup> T-cell infiltration in the leading edge (<i>P</i> < 0.001). There was no relationship between CD64 (a receptor for autoreactive T-cell responses) and CD8<sup>+</sup>/CD4<sup>+</sup> T cells, or between the microglia/macrophage antigen presentation marker HLA-DR and microglial motility (Iba1) in the tumour margins. Natural killer cell infiltration (CD335<sup>+</sup>) correlated with CD8<sup>+</sup> T cells and with CD68/CD163/triggering receptor expressed on myeloid cells 2 anti-inflammatory microglia/macrophages at the leading edge. In an independent large glioblastoma cohort with transcriptomic data, positive correlations between anti-inflammatory microglia/macrophage markers (triggering receptor expressed on myeloid cells 2, CD163 and CD32a) and CD4<sup>+</sup>/CD8<sup>+</sup>/programmed death-ligand 1 RNA expression were validated (<i>P</i> < 0.001). Finally, multivariate analysis showed that high triggering receptor expressed on myeloid cells 2, programmed death-ligand 1 and CD32a expression at the leading edge were significantly associated with poorer overall patient survival (hazard ratio = 2.05, 3.42 and 2.11, respectively), independent of clinical variables. In conclusion, anti-inflammatory microglia/macrophages, CD8<sup>+</sup> T cells and programmed death-ligand 1 are correlated in the invasive margins of glioblastoma, consistent with immune-suppressive interactions. High triggering receptor expressed on myeloid cells 2, programmed death-ligand 1 and CD32a expression at the human glioblastoma leading edge are predictors of poorer overall survival. Given substantial interest in targeting microglia/macrophages, together with immune checkpoint inhibitors in cancer, these data have major clinical implications.</p>","PeriodicalId":9318,"journal":{"name":"Brain Communications","volume":"5 3","pages":"fcad176"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10265726/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/braincomms/fcad176","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
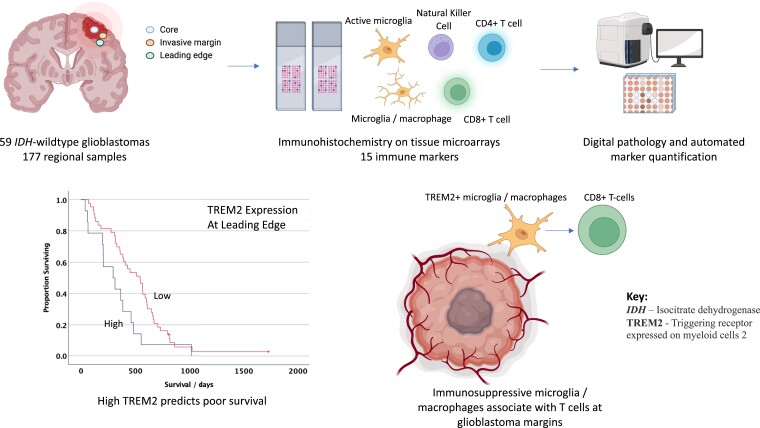
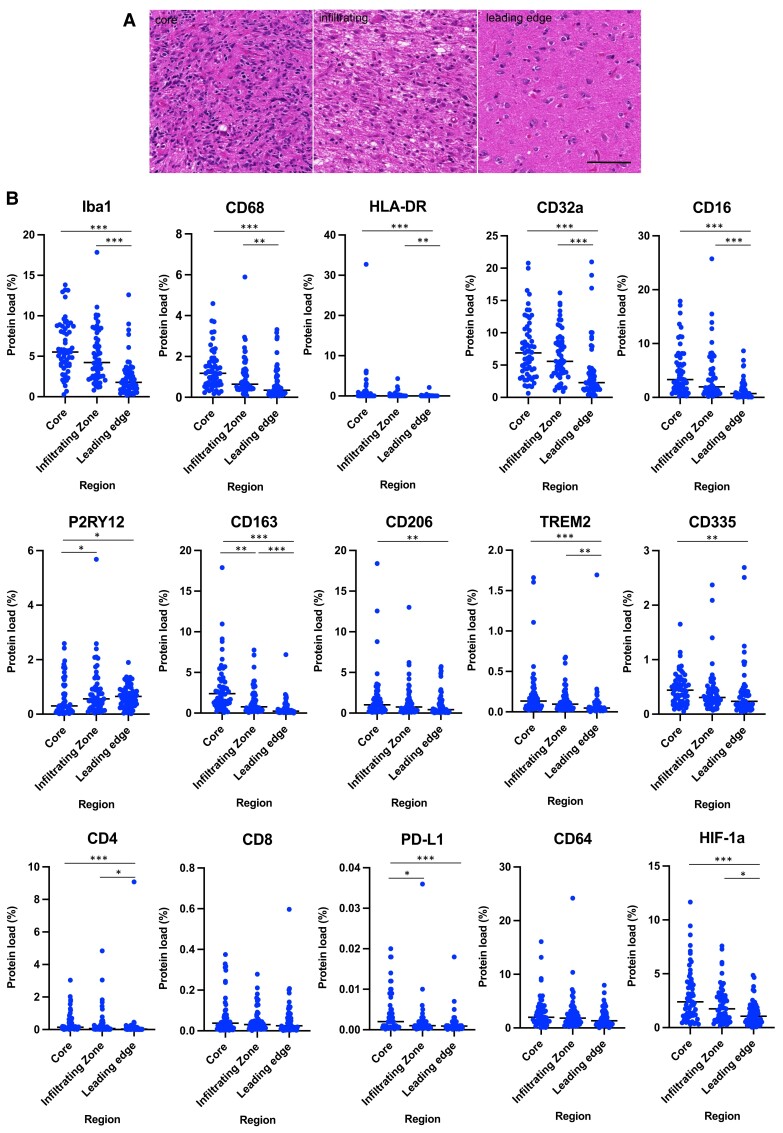
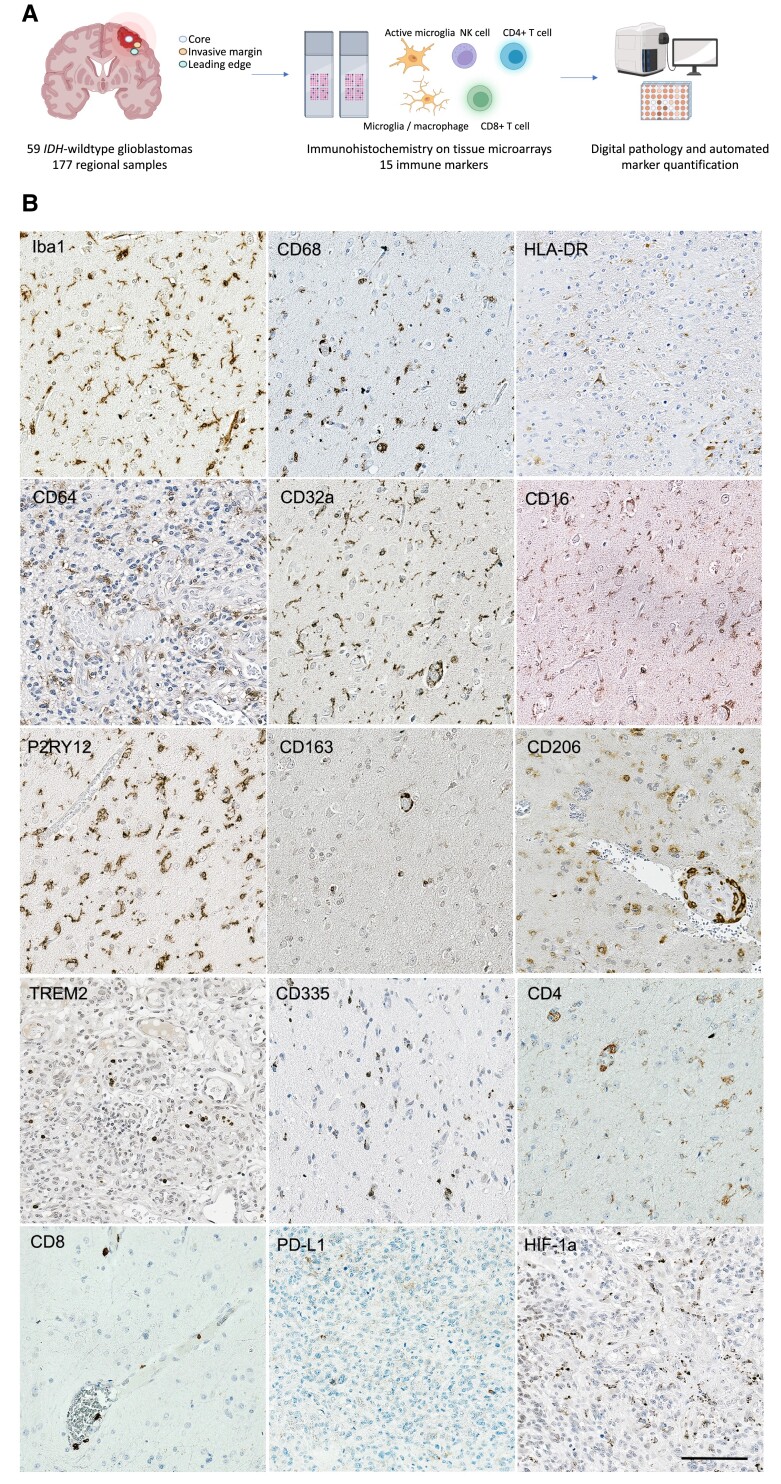
Glioblastoma is a devastating brain cancer for which effective treatments are required. Tumour-associated microglia and macrophages promote glioblastoma growth in an immune-suppressed microenvironment. Most recurrences occur at the invasive margin of the surrounding brain, yet the relationships between microglia/macrophage phenotypes, T cells and programmed death-ligand 1 (an immune checkpoint) across human glioblastoma regions are understudied. In this study, we performed a quantitative immunohistochemical analysis of 15 markers of microglia/macrophage phenotypes (including anti-inflammatory markers triggering receptor expressed on myeloid cells 2 and CD163, and the low-affinity-activating receptor CD32a), T cells, natural killer cells and programmed death-ligand 1, in 59 human IDH1-wild-type glioblastoma multi-regional samples (n = 177; 1 sample at tumour core, 2 samples at the margins: the infiltrating zone and leading edge). Assessment was made for the prognostic value of markers; the results were validated in an independent cohort. Microglia/macrophage motility and activation (Iba1, CD68), programmed death-ligand 1 and CD4+ T cells were reduced, and homeostatic microglia (P2RY12) were increased in the invasive margins compared with the tumour core. There were significant positive correlations between microglia/macrophage markers CD68 (phagocytic)/triggering receptor expressed on myeloid cells 2 (anti-inflammatory) and CD8+ T cells in the invasive margins but not in the tumour core (P < 0.01). Programmed death-ligand 1 expression was associated with microglia/macrophage markers (including anti-inflammatory) CD68, CD163, CD32a and triggering receptor expressed on myeloid cells 2, only in the leading edge of glioblastomas (P < 0.01). Similarly, there was a positive correlation between programmed death-ligand 1 expression and CD8+ T-cell infiltration in the leading edge (P < 0.001). There was no relationship between CD64 (a receptor for autoreactive T-cell responses) and CD8+/CD4+ T cells, or between the microglia/macrophage antigen presentation marker HLA-DR and microglial motility (Iba1) in the tumour margins. Natural killer cell infiltration (CD335+) correlated with CD8+ T cells and with CD68/CD163/triggering receptor expressed on myeloid cells 2 anti-inflammatory microglia/macrophages at the leading edge. In an independent large glioblastoma cohort with transcriptomic data, positive correlations between anti-inflammatory microglia/macrophage markers (triggering receptor expressed on myeloid cells 2, CD163 and CD32a) and CD4+/CD8+/programmed death-ligand 1 RNA expression were validated (P < 0.001). Finally, multivariate analysis showed that high triggering receptor expressed on myeloid cells 2, programmed death-ligand 1 and CD32a expression at the leading edge were significantly associated with poorer overall patient survival (hazard ratio = 2.05, 3.42 and 2.11, respectively), independent of clinical variables. In conclusion, anti-inflammatory microglia/macrophages, CD8+ T cells and programmed death-ligand 1 are correlated in the invasive margins of glioblastoma, consistent with immune-suppressive interactions. High triggering receptor expressed on myeloid cells 2, programmed death-ligand 1 and CD32a expression at the human glioblastoma leading edge are predictors of poorer overall survival. Given substantial interest in targeting microglia/macrophages, together with immune checkpoint inhibitors in cancer, these data have major clinical implications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


