A qualitative investigation of paediatric intensive care staff attitudes towards the diagnosis of lower respiratory tract infection in the molecular diagnostics era.
John A Clark, Andrew Conway Morris, Constantinos Kanaris, David Inwald, Warwick Butt, Joshua Osowicki, Luregn J Schlapbach, Martin D Curran, Deborah White, Esther Daubney, Shruti Agrawal, Vilas Navapurkar, M Estée Török, Stephen Baker, Nazima Pathan
{"title":"A qualitative investigation of paediatric intensive care staff attitudes towards the diagnosis of lower respiratory tract infection in the molecular diagnostics era.","authors":"John A Clark, Andrew Conway Morris, Constantinos Kanaris, David Inwald, Warwick Butt, Joshua Osowicki, Luregn J Schlapbach, Martin D Curran, Deborah White, Esther Daubney, Shruti Agrawal, Vilas Navapurkar, M Estée Török, Stephen Baker, Nazima Pathan","doi":"10.1007/s44253-023-00008-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In the past decade, molecular diagnostic syndromic arrays incorporating a range of bacterial and viral pathogens have been described. It is unclear how paediatric intensive care unit (PICU) staff diagnose lower respiratory tract infection (LRTI) and integrate diagnostic array results into antimicrobial decision-making.</p><p><strong>Methods: </strong>An online survey with eleven questions was distributed throughout paediatric intensive care societies in the UK, continental Europe and Australasia with a total of 755 members. Participants were asked to rate the clinical factors and investigations they used when prescribing for LRTI. Semi-structured interviews were undertaken with staff who participated in a single-centre observational study of a 52-pathogen diagnostic array.</p><p><strong>Results: </strong>Seventy-two survey responses were received; most responses were from senior doctors. Whilst diagnostic arrays were used less frequently than routine investigations (i.e. microbiological culture), they were of comparable perceived utility when making antimicrobial decisions. Prescribers reported that for arrays to be clinically impactful, they would need to deliver results within 6 h for stable patients and within 1 h for unstable patients to inform their immediate decision to prescribe antimicrobials. From 16 staff interviews, we identified that arrays were helpful for the diagnosis and screening of bacterial LRTI. Staff reported it could be challenging to interpret results in some cases due to the high sensitivity of the test. Therefore, results were considered within the context of the patient and discussed within the multidisciplinary team.</p><p><strong>Conclusions: </strong>Diagnostic arrays were considered of comparable value to microbiological investigations by PICU prescribers. Our findings support the need for further clinical and economic evaluation of diagnostic arrays in a randomised control trial.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov, NCT04233268. Registered on 18 January 2020.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s44253-023-00008-z.</p>","PeriodicalId":73402,"journal":{"name":"Intensive care medicine. Paediatric and neonatal","volume":"1 1","pages":"10"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10329081/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive care medicine. Paediatric and neonatal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s44253-023-00008-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/7 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In the past decade, molecular diagnostic syndromic arrays incorporating a range of bacterial and viral pathogens have been described. It is unclear how paediatric intensive care unit (PICU) staff diagnose lower respiratory tract infection (LRTI) and integrate diagnostic array results into antimicrobial decision-making.
Methods: An online survey with eleven questions was distributed throughout paediatric intensive care societies in the UK, continental Europe and Australasia with a total of 755 members. Participants were asked to rate the clinical factors and investigations they used when prescribing for LRTI. Semi-structured interviews were undertaken with staff who participated in a single-centre observational study of a 52-pathogen diagnostic array.
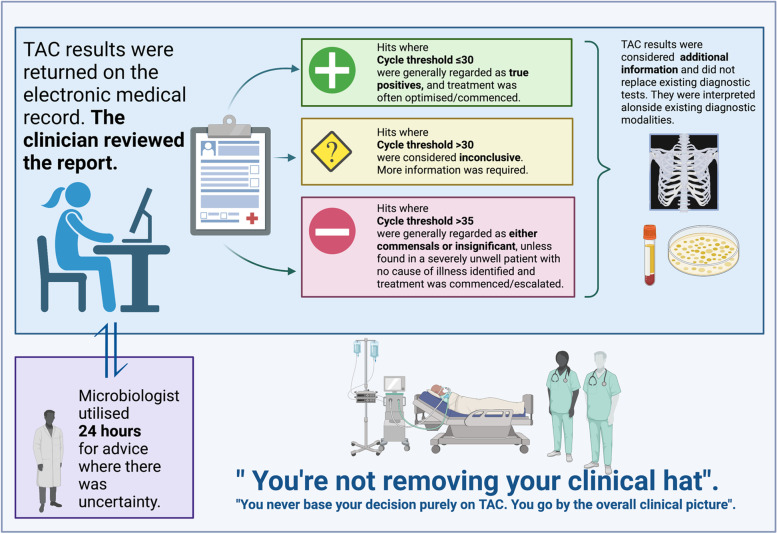
Results: Seventy-two survey responses were received; most responses were from senior doctors. Whilst diagnostic arrays were used less frequently than routine investigations (i.e. microbiological culture), they were of comparable perceived utility when making antimicrobial decisions. Prescribers reported that for arrays to be clinically impactful, they would need to deliver results within 6 h for stable patients and within 1 h for unstable patients to inform their immediate decision to prescribe antimicrobials. From 16 staff interviews, we identified that arrays were helpful for the diagnosis and screening of bacterial LRTI. Staff reported it could be challenging to interpret results in some cases due to the high sensitivity of the test. Therefore, results were considered within the context of the patient and discussed within the multidisciplinary team.
Conclusions: Diagnostic arrays were considered of comparable value to microbiological investigations by PICU prescribers. Our findings support the need for further clinical and economic evaluation of diagnostic arrays in a randomised control trial.
Trial registration: Clinicaltrials.gov, NCT04233268. Registered on 18 January 2020.
Supplementary information: The online version contains supplementary material available at 10.1007/s44253-023-00008-z.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


