Gordonia sputi-associated bloodstream infection in a renal transplant patient with chronic indwelling central venous catheter: a case report and literature review.
Calvin Ka-Fung Lo, Conor Broderick, Aleksandra Stefanovic, William Connors, Melanie Murray
{"title":"<i>Gordonia sputi</i>-associated bloodstream infection in a renal transplant patient with chronic indwelling central venous catheter: a case report and literature review.","authors":"Calvin Ka-Fung Lo, Conor Broderick, Aleksandra Stefanovic, William Connors, Melanie Murray","doi":"10.1099/acmi.0.000560.v3","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Although rare, human infections caused by <i>Gordonia</i> spp. have been reported, especially within the immunocompromised population and those with long-term indwelling devices. We report a case of <i>Gordonia</i> spp. bacteraemia in a renal transplant patient and present a literature review on microbiological identification methods of this organism.</p><p><strong>Case presentation: </strong>A 62-year-old female renal transplant recipient admitted to hospital with a 2-month history of dry cough and fevers occurring weekly when receiving electrolyte replacement infusions via a Groshong line. Over 2 weeks, blood cultures repeatedly isolated a Gram-positive bacillus solely in aerobic bottles, and this was initially reported as <i>Rhodococcus</i> spp. by the local microbiology laboratory. Chest computed tomography (CT) showed multiple ground-glass lung opacities suggestive of septic pulmonary emboli. As central line-associated bloodstream infection was suspected, empirical antibiotics were initiated and the Groshong line was removed. The Gram-positive bacillus was later confirmed by the reference laboratory as <i>Gordonia sputi</i> via 16S rRNA sequencing. Vancomycin and ciprofloxacin for a duration of 6 weeks were completed as targeted antimicrobial therapy. After treatment, the patient remained symptom-free with marked improvement on repeat CT chest imaging.</p><p><strong>Conclusion: </strong>This case illustrates the challenges surrounding identification of <i>Gordonia</i> spp. and other aerobic actinomycetes. 16S rRNA gene sequencing may be a preferred identification method, especially when initial workup of a weakly acid-fast organism fails to make an identification or shows discrepant results using traditional diagnostic modalities.</p>","PeriodicalId":6956,"journal":{"name":"Access Microbiology","volume":"5 6","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10323808/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Access Microbiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1099/acmi.0.000560.v3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Although rare, human infections caused by Gordonia spp. have been reported, especially within the immunocompromised population and those with long-term indwelling devices. We report a case of Gordonia spp. bacteraemia in a renal transplant patient and present a literature review on microbiological identification methods of this organism.
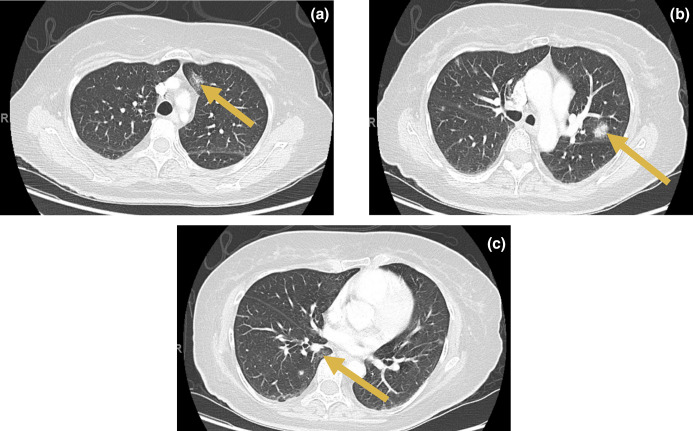
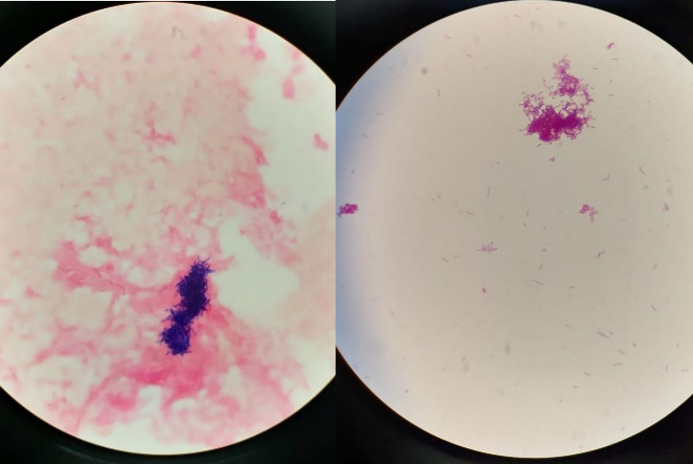
Case presentation: A 62-year-old female renal transplant recipient admitted to hospital with a 2-month history of dry cough and fevers occurring weekly when receiving electrolyte replacement infusions via a Groshong line. Over 2 weeks, blood cultures repeatedly isolated a Gram-positive bacillus solely in aerobic bottles, and this was initially reported as Rhodococcus spp. by the local microbiology laboratory. Chest computed tomography (CT) showed multiple ground-glass lung opacities suggestive of septic pulmonary emboli. As central line-associated bloodstream infection was suspected, empirical antibiotics were initiated and the Groshong line was removed. The Gram-positive bacillus was later confirmed by the reference laboratory as Gordonia sputi via 16S rRNA sequencing. Vancomycin and ciprofloxacin for a duration of 6 weeks were completed as targeted antimicrobial therapy. After treatment, the patient remained symptom-free with marked improvement on repeat CT chest imaging.
Conclusion: This case illustrates the challenges surrounding identification of Gordonia spp. and other aerobic actinomycetes. 16S rRNA gene sequencing may be a preferred identification method, especially when initial workup of a weakly acid-fast organism fails to make an identification or shows discrepant results using traditional diagnostic modalities.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


