Anna Stroud, Pearl Dhaliwal, Richard J Harvey, Raquel Alvarado, Benjamin P Jonker, Mark J Winder, Jessica W Grayson, Ann McCormack
{"title":"Low but not undetectable early postoperative nadir serum cortisol predicts sustained remission in Cushing's disease.","authors":"Anna Stroud, Pearl Dhaliwal, Richard J Harvey, Raquel Alvarado, Benjamin P Jonker, Mark J Winder, Jessica W Grayson, Ann McCormack","doi":"10.1530/EO-21-0026","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Transsphenoidal surgery (TSS) is the first-line treatment for Cushing's disease. The objectives of the study were to determine remission and recurrence rates after TSS for Cushing's disease, identify factors that predict these outcomes, and define the threshold for postoperative morning serum cortisol (MSeC) that most accurately predicts sustained remission.</p><p><strong>Methods: </strong>Records were retrospectively reviewed for consecutive adults undergoing TSS for Cushing's disease at a tertiary centre (1990-2019). Remission was defined as MSeC <138 nmol/L by 6 weeks postoperatively. Recurrence was defined as elevated 24-h urine free cortisol, lack of suppression after dexamethasone or elevated midnight salivary cortisol.</p><p><strong>Results: </strong>In this study, 42 patients (age 47 ± 13 years, 83% female) were assessed with 55 ± 56 months of follow-up. Remission occurred after 77% of primary (<i>n</i> = 30) and 42% of revision operations (<i>n</i> = 12). After primary surgery, remission was associated with lower MSeC nadir (26 ± 36 nmol/L vs 347 ± 220 nmol/L, <i>P</i> < 0.01) and lower adrenocorticotropin nadir (2 ± 3 pmol/L vs 6 ± 3 pmol/L, <i>P</i> = 0.01). Sustained remission 5 years after surgery was predicted by MSeC <92 nmol/L within 2 weeks postoperatively (sensitivity 100% and specificity 100%). After revision surgery, remission was predicted by lower MSeC nadir (70 ± 45 nmol/L vs 408 ± 305 nmol/L, <i>P</i> = 0.03), smaller tumour diameter (3 ± 2 mm vs 15 ± 13 mm, <i>P</i> = 0.05) and absence of cavernous sinus invasion (0% vs 71%, <i>P</i> = 0.03). Recurrence after primary and revision surgery occurred in 17% and 20% of patients respectively.</p><p><strong>Conclusions: </strong>Lower postoperative MSeC nadir strongly predicted remission after both primary and revision surgery. Following primary surgery, an MSeC <92 nmol/L within 2 weeks predicted sustained remission at 5 years. MSeC nadir was the most important prognostic marker following TSS for Cushing's disease.</p>","PeriodicalId":72907,"journal":{"name":"Endocrine oncology (Bristol, England)","volume":"2 1","pages":"19-31"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10259300/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine oncology (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EO-21-0026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Transsphenoidal surgery (TSS) is the first-line treatment for Cushing's disease. The objectives of the study were to determine remission and recurrence rates after TSS for Cushing's disease, identify factors that predict these outcomes, and define the threshold for postoperative morning serum cortisol (MSeC) that most accurately predicts sustained remission.
Methods: Records were retrospectively reviewed for consecutive adults undergoing TSS for Cushing's disease at a tertiary centre (1990-2019). Remission was defined as MSeC <138 nmol/L by 6 weeks postoperatively. Recurrence was defined as elevated 24-h urine free cortisol, lack of suppression after dexamethasone or elevated midnight salivary cortisol.
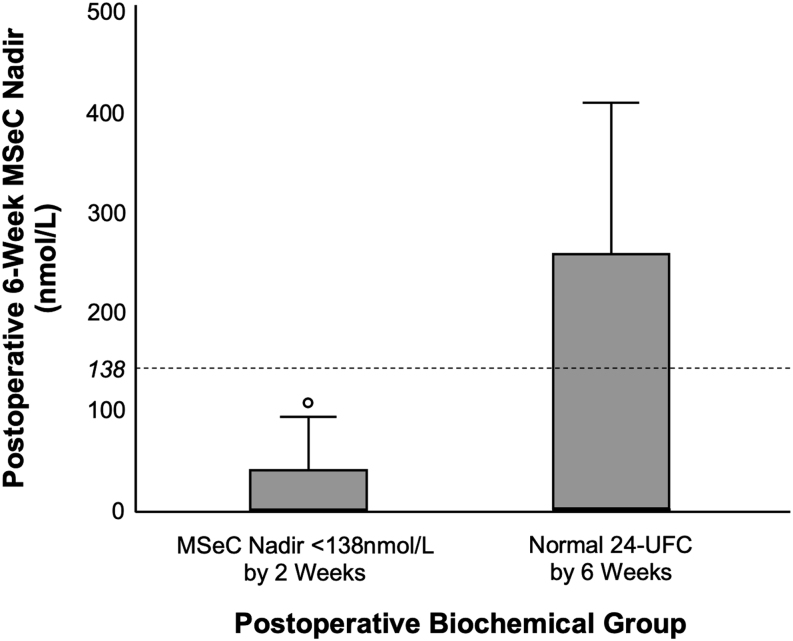
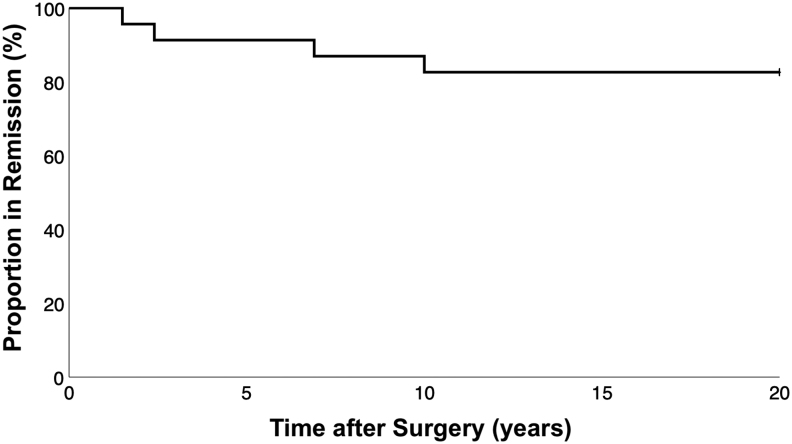
Results: In this study, 42 patients (age 47 ± 13 years, 83% female) were assessed with 55 ± 56 months of follow-up. Remission occurred after 77% of primary (n = 30) and 42% of revision operations (n = 12). After primary surgery, remission was associated with lower MSeC nadir (26 ± 36 nmol/L vs 347 ± 220 nmol/L, P < 0.01) and lower adrenocorticotropin nadir (2 ± 3 pmol/L vs 6 ± 3 pmol/L, P = 0.01). Sustained remission 5 years after surgery was predicted by MSeC <92 nmol/L within 2 weeks postoperatively (sensitivity 100% and specificity 100%). After revision surgery, remission was predicted by lower MSeC nadir (70 ± 45 nmol/L vs 408 ± 305 nmol/L, P = 0.03), smaller tumour diameter (3 ± 2 mm vs 15 ± 13 mm, P = 0.05) and absence of cavernous sinus invasion (0% vs 71%, P = 0.03). Recurrence after primary and revision surgery occurred in 17% and 20% of patients respectively.
Conclusions: Lower postoperative MSeC nadir strongly predicted remission after both primary and revision surgery. Following primary surgery, an MSeC <92 nmol/L within 2 weeks predicted sustained remission at 5 years. MSeC nadir was the most important prognostic marker following TSS for Cushing's disease.
目的:经蝶窦手术(TSS)是库欣病的一线治疗方法。本研究的目的是确定库欣病TSS后的缓解率和复发率,确定预测这些结果的因素,并确定最准确预测持续缓解的术后早晨血清皮质醇(MSeC)阈值。方法:回顾性分析1990-2019年在三级医疗中心连续接受库欣病TSS治疗的成年人的记录。结果:在这项研究中,42例患者(年龄47±13岁,83%为女性)在55±56个月的随访中被评估。77%的原发性手术(n = 30)和42%的翻修手术(n = 12)缓解。原发性手术后,缓解与较低的MSeC最低点(26±36 nmol/L vs 347±220 nmol/L, P < 0.01)和较低的促肾上腺皮质激素最低点(2±3 pmol/L vs 6±3 pmol/L, P = 0.01)相关。MSeC (P = 0.03)、肿瘤直径较小(3±2mm vs 15±13mm, P = 0.05)和海绵窦无侵犯(0% vs 71%, P = 0.03)预测术后5年持续缓解。初次手术和翻修手术后的复发率分别为17%和20%。结论:较低的术后MSeC最低点强烈预测了初次手术和翻修手术后的缓解。初次手术后,进行MSeC


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


