Hani Chanbour, Patrick D Kelly, Michael C Topf, Michael C Dewan, Peter J Morone, Scott L Zuckerman
{"title":"Resection of a ventral intramedullary spinal cord ependymoma through an anterior cervical approach: illustrative case.","authors":"Hani Chanbour, Patrick D Kelly, Michael C Topf, Michael C Dewan, Peter J Morone, Scott L Zuckerman","doi":"10.3171/CASE23243","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although posterior myelotomy leaves patients with dorsal column deficits, few reports have explored the anterior cervical approach for cervical intramedullary tumors. The authors describe the resection of a cervical intramedullary ependymoma through an anterior approach with a two-level corpectomy and fusion.</p><p><strong>Observations: </strong>A 49-year-old male presented with a C3-5 ventral intramedullary mass with polar cysts. Because of the ventral location of the tumor and the added benefit of avoiding a posterior myelotomy and dorsal column deficits, an anterior C4-5 corpectomy offered a direct route and excellent visualization of the ventrally located tumor. After a C4-5 corpectomy, microsurgical resection, and C3-6 anterior fusion with a fibular allograft filled with autograft, the patient remained neurologically intact. Magnetic resonance imaging (MRI) on postoperative day (POD) 1 confirmed gross-total resection. The patient was extubated on POD 2 and was discharged home on POD 4 with a stable examination. At 9 months, the patient developed mechanical neck pain refractory to conservative treatment and underwent a posterior fusion to address pseudarthrosis. MRI at 15 months showed no evidence of tumor recurrence with the resolution of neck pain.</p><p><strong>Lessons: </strong>An anterior cervical corpectomy provides a safe corridor to access ventral cervical intramedullary tumors and avoids posterior myelotomy. Although the patient required a three-level fusion, we believe the tradeoff of decreased motion compared to dorsal column deficits is preferred.</p>","PeriodicalId":16554,"journal":{"name":"Journal of Neurosurgery: Case Lessons","volume":"6 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cf/0d/CASE23243.PMC10555634.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurosurgery: Case Lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE23243","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Although posterior myelotomy leaves patients with dorsal column deficits, few reports have explored the anterior cervical approach for cervical intramedullary tumors. The authors describe the resection of a cervical intramedullary ependymoma through an anterior approach with a two-level corpectomy and fusion.
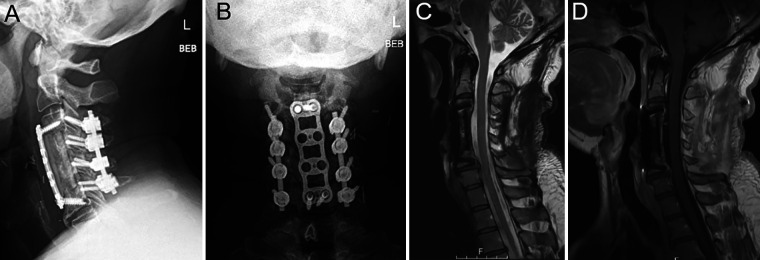
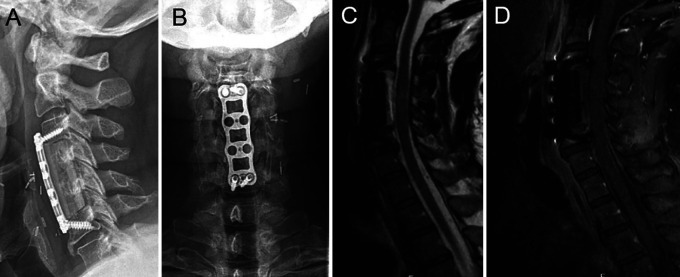
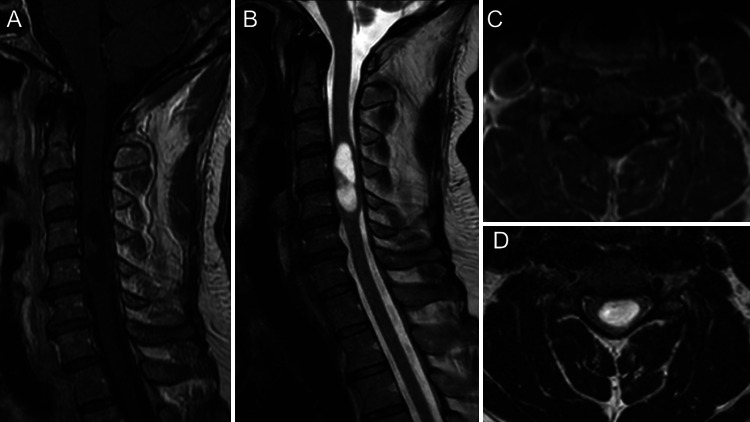
Observations: A 49-year-old male presented with a C3-5 ventral intramedullary mass with polar cysts. Because of the ventral location of the tumor and the added benefit of avoiding a posterior myelotomy and dorsal column deficits, an anterior C4-5 corpectomy offered a direct route and excellent visualization of the ventrally located tumor. After a C4-5 corpectomy, microsurgical resection, and C3-6 anterior fusion with a fibular allograft filled with autograft, the patient remained neurologically intact. Magnetic resonance imaging (MRI) on postoperative day (POD) 1 confirmed gross-total resection. The patient was extubated on POD 2 and was discharged home on POD 4 with a stable examination. At 9 months, the patient developed mechanical neck pain refractory to conservative treatment and underwent a posterior fusion to address pseudarthrosis. MRI at 15 months showed no evidence of tumor recurrence with the resolution of neck pain.
Lessons: An anterior cervical corpectomy provides a safe corridor to access ventral cervical intramedullary tumors and avoids posterior myelotomy. Although the patient required a three-level fusion, we believe the tradeoff of decreased motion compared to dorsal column deficits is preferred.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


