Joshua Xu, Ewout S Veltman, Yuan Chai, William L Walter
{"title":"Accuracy of acetabular component alignment with surgical guidance systems during hip arthroplasty.","authors":"Joshua Xu, Ewout S Veltman, Yuan Chai, William L Walter","doi":"10.1051/sicotj/2023010","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Navigation in total hip arthroplasty has been shown to improve acetabular positioning and can decrease the incidence of mal-positioned acetabular components. This study aimed to assess two surgical guidance systems by comparing intra-operative measurements of acetabular component inclination and anteversion with a post-operative CT scan.</p><p><strong>Methods: </strong>We prospectively collected intra-operative navigation data from 102 hips receiving conventional THA or hip resurfacing arthroplasty through either a direct anterior or posterior approach. Two guidance systems were used simultaneously: an inertial navigation system (INS) and an optical navigation system (ONS). Acetabular component anteversion and inclination were measured on a post-operative CT.</p><p><strong>Results: </strong>The average age of the patients was 64 years (range: 24-92) and the average BMI was 27 kg/m<sup>2</sup> (range 19-38). 52% had hip surgery through an anterior approach. 98% of the INS measurements and 88% of the ONS measurements were within 10° of the CT measurements. The mean (and standard deviation) of the absolute difference between the postoperative CT and the intra-operative measurements for inclination and anteversion were 3.0° (2.8) and 4.5° (3.2) respectively for the ONS, along with 2.1° (2.3) and 2.4° (2.1) respectively for the INS. There was a significantly lower mean absolute difference to CT for the INS when compared to ONS in both anteversions (p < 0.001) and inclination (p = 0.02).</p><p><strong>Conclusions: </strong>We found that both inertial and optical navigation systems allowed for adequate acetabular positioning as measured on postoperative CT, and thus provide reliable intraoperative feedback for optimal acetabular component placement.</p><p><strong>Level of evidence: </strong>Therapeutic Level II.</p>","PeriodicalId":46378,"journal":{"name":"SICOT-J","volume":"9 ","pages":"12"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10161875/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SICOT-J","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1051/sicotj/2023010","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Navigation in total hip arthroplasty has been shown to improve acetabular positioning and can decrease the incidence of mal-positioned acetabular components. This study aimed to assess two surgical guidance systems by comparing intra-operative measurements of acetabular component inclination and anteversion with a post-operative CT scan.
Methods: We prospectively collected intra-operative navigation data from 102 hips receiving conventional THA or hip resurfacing arthroplasty through either a direct anterior or posterior approach. Two guidance systems were used simultaneously: an inertial navigation system (INS) and an optical navigation system (ONS). Acetabular component anteversion and inclination were measured on a post-operative CT.
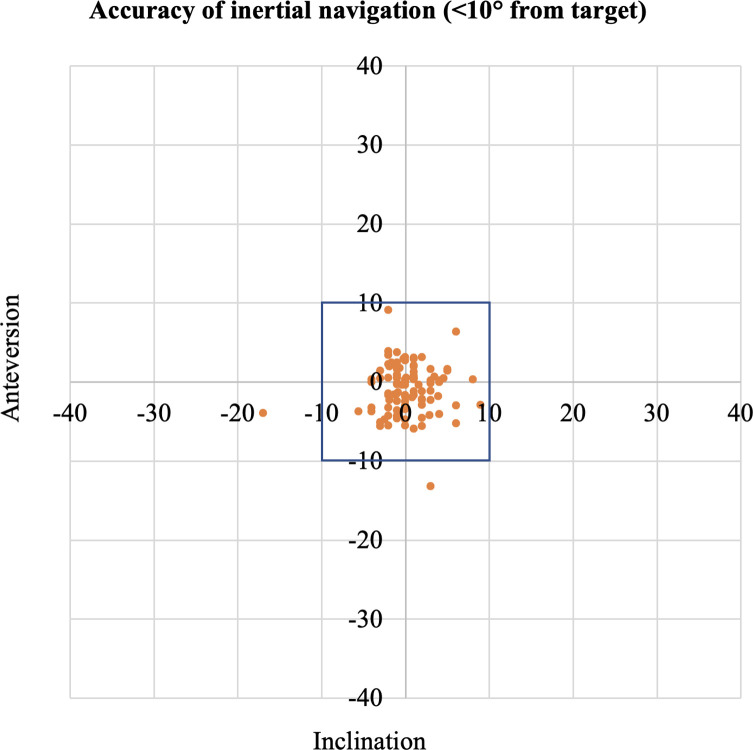
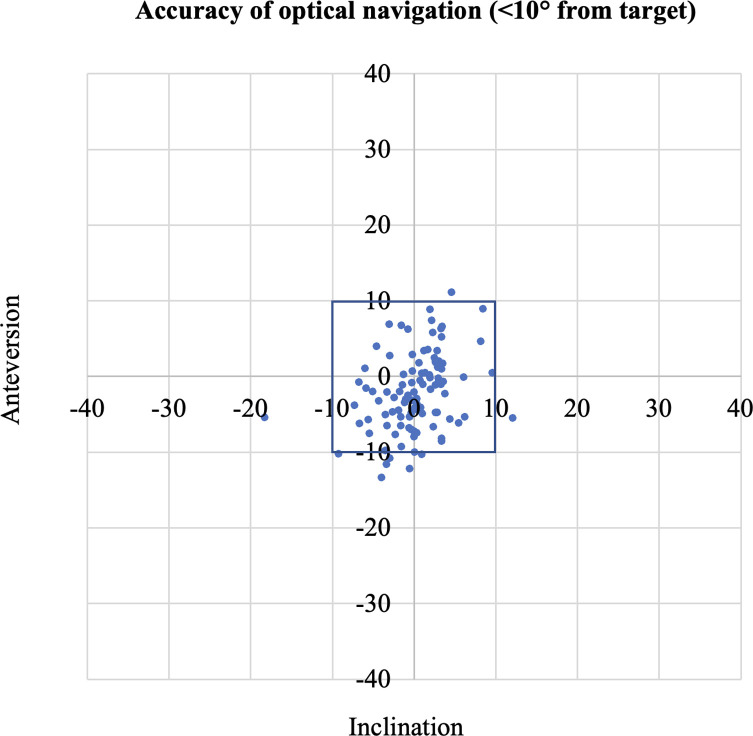
Results: The average age of the patients was 64 years (range: 24-92) and the average BMI was 27 kg/m2 (range 19-38). 52% had hip surgery through an anterior approach. 98% of the INS measurements and 88% of the ONS measurements were within 10° of the CT measurements. The mean (and standard deviation) of the absolute difference between the postoperative CT and the intra-operative measurements for inclination and anteversion were 3.0° (2.8) and 4.5° (3.2) respectively for the ONS, along with 2.1° (2.3) and 2.4° (2.1) respectively for the INS. There was a significantly lower mean absolute difference to CT for the INS when compared to ONS in both anteversions (p < 0.001) and inclination (p = 0.02).
Conclusions: We found that both inertial and optical navigation systems allowed for adequate acetabular positioning as measured on postoperative CT, and thus provide reliable intraoperative feedback for optimal acetabular component placement.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


