Ahmad R Masri, Bailey R Yekzaman, Bradley J Estes, Christopher S Park, Patrick Landazuri, Michael Kinsman
{"title":"Infraclavicular de novo placement of a responsive neurostimulator for a patient with eloquent glioma-associated epilepsy: illustrative case.","authors":"Ahmad R Masri, Bailey R Yekzaman, Bradley J Estes, Christopher S Park, Patrick Landazuri, Michael Kinsman","doi":"10.3171/CASE22528","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The authors present a 50-year-old female with high-grade glioma involving the motor cortex as the cause of her drug-resistant epilepsy (DRE). Responsive neurostimulation (RNS) was chosen for epilepsy treatment. Due to concerns regarding the generator impeding the regular imaging surveillance required for treatment and monitoring of her glioma, surgeons placed the internal pulse generator (IPG) within an infraclavicular chest pocket.</p><p><strong>Observations: </strong>Implantation of the RNS device and IPG within the infraclavicular pocket was uneventful. However, both subdural and depth electrodes were used and connected to the IPG, and subdural electrodes are considerably shorter than depth electrodes (37 vs 44 cm). The shorter strip leads presumably generated significant tension, leading to fracture of the leads. Therefore, surgery was repeated using only depth electrodes for more length and less tension. The device has good-quality electrocorticography signals that continue to be used for device programming. The seizure burden was reduced, and quality of life improved for the patient.</p><p><strong>Lessons: </strong>The RNS system with infraclavicular IPG placement reduced the seizure burden and improved the quality of life of a patient with glioma-associated epilepsy. Surgeons may consider the infraclavicular location as an alternative site for implantation for RNS candidates who require recurrent intracranial magnetic resonance imaging.</p>","PeriodicalId":16554,"journal":{"name":"Journal of Neurosurgery: Case Lessons","volume":"5 26","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a2/ce/CASE22528.PMC10550545.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurosurgery: Case Lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE22528","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
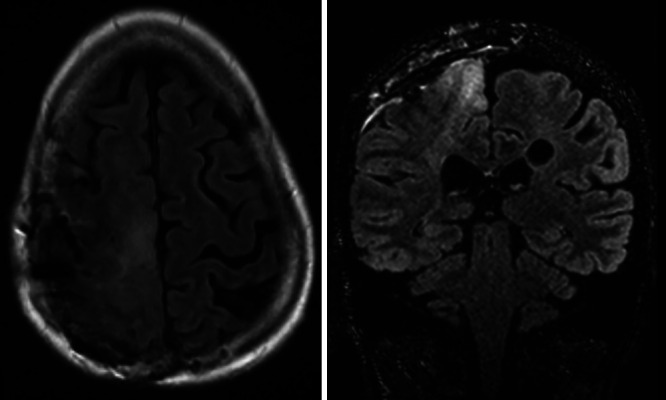
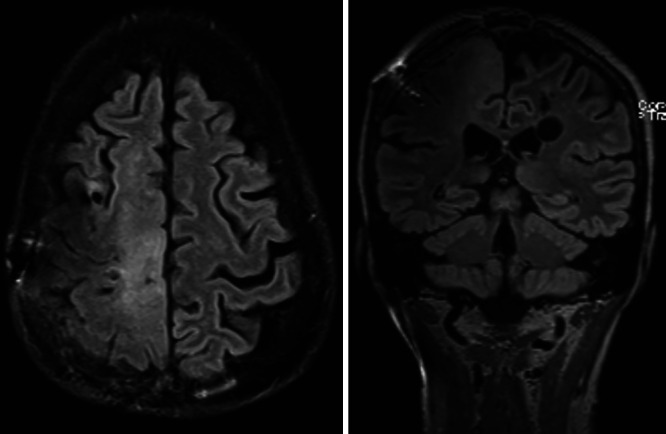
Background: The authors present a 50-year-old female with high-grade glioma involving the motor cortex as the cause of her drug-resistant epilepsy (DRE). Responsive neurostimulation (RNS) was chosen for epilepsy treatment. Due to concerns regarding the generator impeding the regular imaging surveillance required for treatment and monitoring of her glioma, surgeons placed the internal pulse generator (IPG) within an infraclavicular chest pocket.
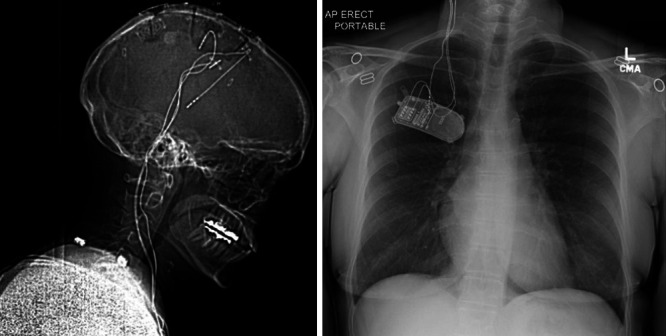
Observations: Implantation of the RNS device and IPG within the infraclavicular pocket was uneventful. However, both subdural and depth electrodes were used and connected to the IPG, and subdural electrodes are considerably shorter than depth electrodes (37 vs 44 cm). The shorter strip leads presumably generated significant tension, leading to fracture of the leads. Therefore, surgery was repeated using only depth electrodes for more length and less tension. The device has good-quality electrocorticography signals that continue to be used for device programming. The seizure burden was reduced, and quality of life improved for the patient.
Lessons: The RNS system with infraclavicular IPG placement reduced the seizure burden and improved the quality of life of a patient with glioma-associated epilepsy. Surgeons may consider the infraclavicular location as an alternative site for implantation for RNS candidates who require recurrent intracranial magnetic resonance imaging.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


