Systemic Nonsteroidal Anti-Inflammatories for Analgesia in Postoperative Critical Care Patients: A Systematic Review and Meta-Analysis of Randomized Control Trials.
Chen Hsiang Ma, Kimberly B Tworek, Janice Y Kung, Sebastian Kilcommons, Kathleen Wheeler, Arabesque Parker, Janek Senaratne, Erika Macintyre, Wendy Sligl, Constantine J Karvellas, Fernando G Zampieri, Demetrios Jim Kutsogiannis, John Basmaji, Kimberley Lewis, Dipayan Chaudhuri, Sameer Sharif, Oleksa G Rewa, Bram Rochwerg, Sean M Bagshaw, Vincent I Lau
{"title":"Systemic Nonsteroidal Anti-Inflammatories for Analgesia in Postoperative Critical Care Patients: A Systematic Review and Meta-Analysis of Randomized Control Trials.","authors":"Chen Hsiang Ma, Kimberly B Tworek, Janice Y Kung, Sebastian Kilcommons, Kathleen Wheeler, Arabesque Parker, Janek Senaratne, Erika Macintyre, Wendy Sligl, Constantine J Karvellas, Fernando G Zampieri, Demetrios Jim Kutsogiannis, John Basmaji, Kimberley Lewis, Dipayan Chaudhuri, Sameer Sharif, Oleksa G Rewa, Bram Rochwerg, Sean M Bagshaw, Vincent I Lau","doi":"10.1097/CCE.0000000000000938","DOIUrl":null,"url":null,"abstract":"<p><p>While opioids are part of usual care for analgesia in the ICU, there are concerns regarding excess use. This is a systematic review of nonsteroidal anti-inflammatory drugs (NSAIDs) use in postoperative critical care adult patients.</p><p><strong>Data sources: </strong>We searched Medical Literature Analysis and Retrieval System Online, Excerpta Medica database, Cumulative Index to Nursing and Allied Health Literature, Cochrane Library, trial registries, Google Scholar, and relevant systematic reviews through March 2023.</p><p><strong>Study selection: </strong>Titles, abstracts, and full texts were reviewed independently and induplicate by two investigators to identify eligible studies. We included randomized control trials (RCTs) that compared NSAIDs alone or as an adjunct to opioids for systemic analgesia. The primary outcome was opioid utilization.</p><p><strong>Data extraction: </strong>In duplicate, investigators independently extracted study characteristics, patient demographics, intervention details, and outcomes of interest using predefined abstraction forms. Statistical analyses were conducted using Review Manager software Version 5.4. (The Cochrane Collaboration, Copenhagen, Denmark).</p><p><strong>Data synthesis: </strong>We included 15 RCTs (<i>n</i> = 1,621 patients) for admission to the ICU for postoperative management after elective procedures. Adjunctive NSAID therapy to opioids reduced 24-hour oral morphine equivalent consumption by 21.4 mg (95% CI, 11.8-31.0 mg reduction; high certainty) and probably reduced pain scores (measured by Visual Analog Scale) by 6.1 mm (95% CI, 12.2 decrease to 0.1 increase; moderate certainty). Adjunctive NSAID therapy probably had no impact on the duration of mechanical ventilation (1.6 hr reduction; 95% CI, 0.4 hr to 2.7 reduction; moderate certainty) and may have no impact on ICU length of stay (2.1 hr reduction; 95% CI, 6.1 hr reduction to 2.0 hr increase; low certainty). Variability in reporting adverse outcomes (e.g., gastrointestinal bleeding, acute kidney injury) precluded their meta-analysis.</p><p><strong>Conclusions: </strong>In postoperative critical care adult patients, systemic NSAIDs reduced opioid use and probably reduced pain scores. However, the evidence is uncertain for the duration of mechanical ventilation or ICU length of stay. Further research is required to characterize the prevalence of NSAID-related adverse outcomes.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 7","pages":"e0938"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/02/98/cc9-5-e0938.PMC10309528.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000938","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
While opioids are part of usual care for analgesia in the ICU, there are concerns regarding excess use. This is a systematic review of nonsteroidal anti-inflammatory drugs (NSAIDs) use in postoperative critical care adult patients.
Data sources: We searched Medical Literature Analysis and Retrieval System Online, Excerpta Medica database, Cumulative Index to Nursing and Allied Health Literature, Cochrane Library, trial registries, Google Scholar, and relevant systematic reviews through March 2023.
Study selection: Titles, abstracts, and full texts were reviewed independently and induplicate by two investigators to identify eligible studies. We included randomized control trials (RCTs) that compared NSAIDs alone or as an adjunct to opioids for systemic analgesia. The primary outcome was opioid utilization.
Data extraction: In duplicate, investigators independently extracted study characteristics, patient demographics, intervention details, and outcomes of interest using predefined abstraction forms. Statistical analyses were conducted using Review Manager software Version 5.4. (The Cochrane Collaboration, Copenhagen, Denmark).
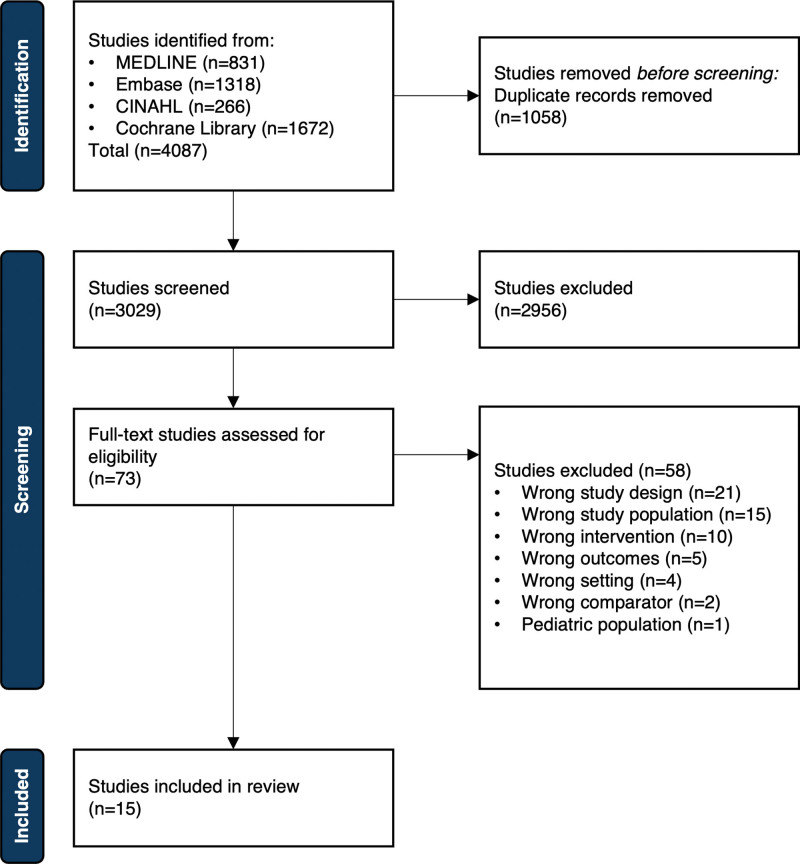
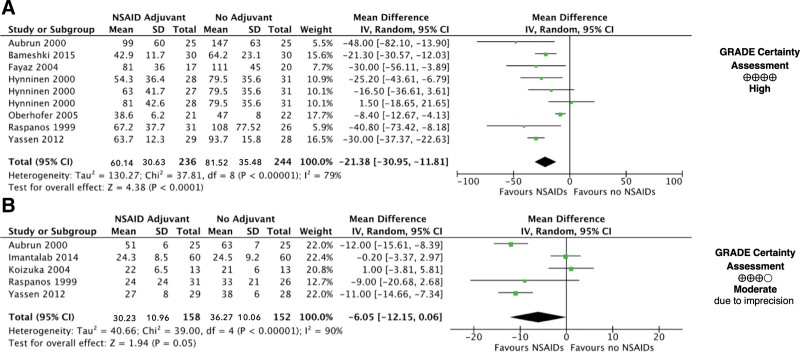
Data synthesis: We included 15 RCTs (n = 1,621 patients) for admission to the ICU for postoperative management after elective procedures. Adjunctive NSAID therapy to opioids reduced 24-hour oral morphine equivalent consumption by 21.4 mg (95% CI, 11.8-31.0 mg reduction; high certainty) and probably reduced pain scores (measured by Visual Analog Scale) by 6.1 mm (95% CI, 12.2 decrease to 0.1 increase; moderate certainty). Adjunctive NSAID therapy probably had no impact on the duration of mechanical ventilation (1.6 hr reduction; 95% CI, 0.4 hr to 2.7 reduction; moderate certainty) and may have no impact on ICU length of stay (2.1 hr reduction; 95% CI, 6.1 hr reduction to 2.0 hr increase; low certainty). Variability in reporting adverse outcomes (e.g., gastrointestinal bleeding, acute kidney injury) precluded their meta-analysis.
Conclusions: In postoperative critical care adult patients, systemic NSAIDs reduced opioid use and probably reduced pain scores. However, the evidence is uncertain for the duration of mechanical ventilation or ICU length of stay. Further research is required to characterize the prevalence of NSAID-related adverse outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


