Ubong Silas, Maximilian Blüher, Antonia Bosworth Smith, Rhodri Saunders
{"title":"Fast In-House Next-Generation Sequencing in the Diagnosis of Metastatic Non-small Cell Lung Cancer: A Hospital Budget Impact Analysis.","authors":"Ubong Silas, Maximilian Blüher, Antonia Bosworth Smith, Rhodri Saunders","doi":"10.36469/001c.77686","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Targeted therapy for cancer is becoming more frequent as the understanding of the molecular pathogenesis increases. Molecular testing must be done to use targeted therapy. Unfortunately, the testing turnaround time can delay the initiation of targeted therapy. <b>Objective:</b> To investigate the impact of a next-generation sequencing (NGS) machine in the hospital that would allow for in-house NGS testing of metastatic non-small cell lung cancer (mNSCLC) in a US setting. <b>Methods:</b> The differences between 2 hospital pathways were established with a cohort-level decision tree that feeds into a Markov model. A pathway that used in-house NGS (75%) and the use of external laboratories (so-called send-out NGS) (25%), was compared with the standard of exclusively send-out NGS. The model was from the perspective of a US hospital over a 5-year time horizon. All cost input data were in or inflated to 2021 USD. Scenario analysis was done on key variables. <b>Results:</b> In a hospital with 500 mNSCLC patients, the implementation of in-house NGS was estimated to increase the testing costs and the revenue of the hospital. The model predicted a $710 060 increase in testing costs, a $1 732 506 increase in revenue, and a $1 022 446 return on investment over 5 years. The payback period was 15 months with in-house NGS. The number of patients on targeted therapy increased by 3.38%, and the average turnaround time decreased by 10 days when in-house NGS was used. <b>Discussion:</b> Reducing testing turnaround time is a benefit of in-house NGS. It could contribute to fewer mNSCLC patients lost to second opinion and an increased number of patients on targeted therapy. The model outcomes predicted that, over a 5-year period, there would be a positive return on investment for a US hospital. The model reflects a proposed scenario. The heterogeneity of hospital inputs and the cost of send-out NGS means context-specific inputs are needed. <b>Conclusion:</b> Using in-house NGS testing could reduce the testing turnaround time and increase the number of patients on targeted therapy. Additional benefits for the hospital are that fewer patients will be lost to second opinion and that in-house NGS could generate additional revenue.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"10 1","pages":"111-118"},"PeriodicalIF":2.3000,"publicationDate":"2023-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10306161/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.77686","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
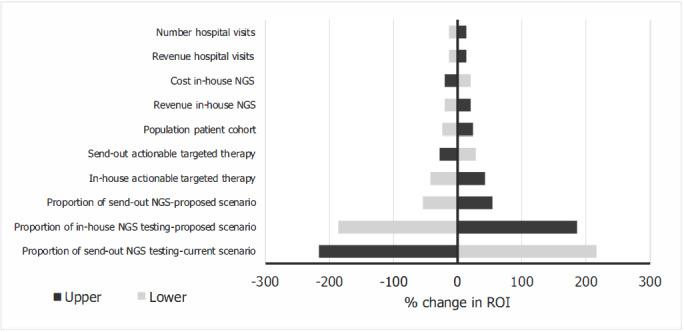
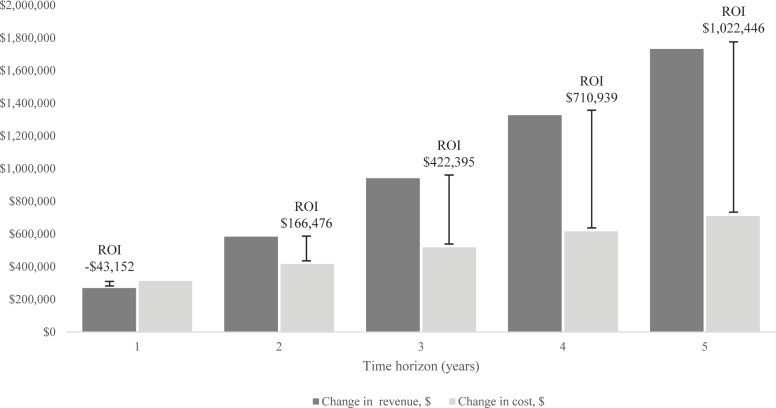
Background: Targeted therapy for cancer is becoming more frequent as the understanding of the molecular pathogenesis increases. Molecular testing must be done to use targeted therapy. Unfortunately, the testing turnaround time can delay the initiation of targeted therapy. Objective: To investigate the impact of a next-generation sequencing (NGS) machine in the hospital that would allow for in-house NGS testing of metastatic non-small cell lung cancer (mNSCLC) in a US setting. Methods: The differences between 2 hospital pathways were established with a cohort-level decision tree that feeds into a Markov model. A pathway that used in-house NGS (75%) and the use of external laboratories (so-called send-out NGS) (25%), was compared with the standard of exclusively send-out NGS. The model was from the perspective of a US hospital over a 5-year time horizon. All cost input data were in or inflated to 2021 USD. Scenario analysis was done on key variables. Results: In a hospital with 500 mNSCLC patients, the implementation of in-house NGS was estimated to increase the testing costs and the revenue of the hospital. The model predicted a $710 060 increase in testing costs, a $1 732 506 increase in revenue, and a $1 022 446 return on investment over 5 years. The payback period was 15 months with in-house NGS. The number of patients on targeted therapy increased by 3.38%, and the average turnaround time decreased by 10 days when in-house NGS was used. Discussion: Reducing testing turnaround time is a benefit of in-house NGS. It could contribute to fewer mNSCLC patients lost to second opinion and an increased number of patients on targeted therapy. The model outcomes predicted that, over a 5-year period, there would be a positive return on investment for a US hospital. The model reflects a proposed scenario. The heterogeneity of hospital inputs and the cost of send-out NGS means context-specific inputs are needed. Conclusion: Using in-house NGS testing could reduce the testing turnaround time and increase the number of patients on targeted therapy. Additional benefits for the hospital are that fewer patients will be lost to second opinion and that in-house NGS could generate additional revenue.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


