Shin Hwang, Ki-Hun Kim, Deok-Bog Moon, Chul-Soo Ahn, Tae-Yong Ha, Gi-Won Song, Dong-Hwan Jung, Gil-Chun Park
{"title":"Prediction of Post-resection Prognosis Using the ADV Score for Huge Hepatocellular Carcinomas ≥13 cm.","authors":"Shin Hwang, Ki-Hun Kim, Deok-Bog Moon, Chul-Soo Ahn, Tae-Yong Ha, Gi-Won Song, Dong-Hwan Jung, Gil-Chun Park","doi":"10.17998/jlc.21.1.45","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aims: </strong>Multiplication of α-fetoprotein, des-γ-carboxy prothrombin, and tumor volume (ADV score) is a surrogate marker for post-resection prognosis of hepatocellular carcinoma (HCC). This study aimed to validate the predictive power of the ADV score-based prognostic prediction model for patients with solitary huge HCC.</p><p><strong>Methods: </strong>Of 3,018 patients, 100 patients who underwent hepatic resection for solitary HCC ≥13 cm between 2008 and 2012 were selected.</p><p><strong>Results: </strong>The median tumor diameter and tumor volume were 15.0 cm and 886 mL, respectively. Tumor recurrence and overall survival (OS) rates were 70.7% and 66.0% at one year and 84.9% and 34.0% at five years, respectively. Microvascular invasion (MVI) was the only independent risk factor for disease-free survival (DFS) and OS. DFS and OS, stratified by ADV score with 1-log intervals, showed significant prognostic contrasts (<i>P</i>=0.007 and <i>P</i>=0.017, respectively). DFS and OS, stratified by ADV score with a cut-off of 8-log, showed significant prognostic contrasts (<i>P</i>=0.014 and <i>P</i>=0.042, respectively). The combination of MVI and ADV score with a cut-off of 8-log also showed significant prognostic contrasts in DFS (<i>P</i><0.001) and OS (<i>P</i>=0.001) considering the number of risk factors. Prognostic contrast was enhanced after combining the MVI and ADV score.</p><p><strong>Conclusions: </strong>The prognostic prediction model with the ADV score could reliably predict the risk of tumor recurrence and long-term patient survival outcomes in patients with solitary huge HCC ≥13 cm. The results of this study suggest that our prognostic prediction models can be used to guide surgical treatment and post-resection follow-up for patients with huge HCCs.</p>","PeriodicalId":16226,"journal":{"name":"Journal of Liver Cancer","volume":"21 1","pages":"45-57"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/4b/jlc-21-1-45.PMC10035719.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Liver Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17998/jlc.21.1.45","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aims: Multiplication of α-fetoprotein, des-γ-carboxy prothrombin, and tumor volume (ADV score) is a surrogate marker for post-resection prognosis of hepatocellular carcinoma (HCC). This study aimed to validate the predictive power of the ADV score-based prognostic prediction model for patients with solitary huge HCC.
Methods: Of 3,018 patients, 100 patients who underwent hepatic resection for solitary HCC ≥13 cm between 2008 and 2012 were selected.
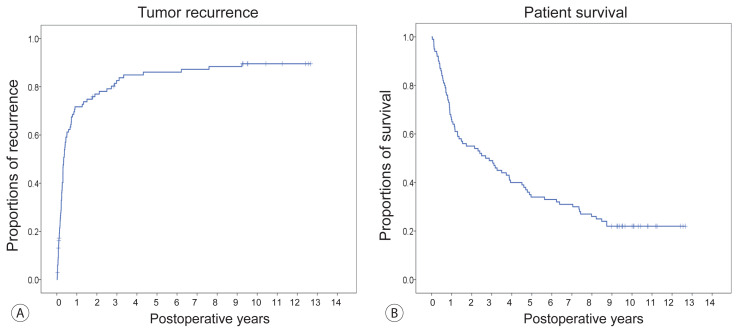
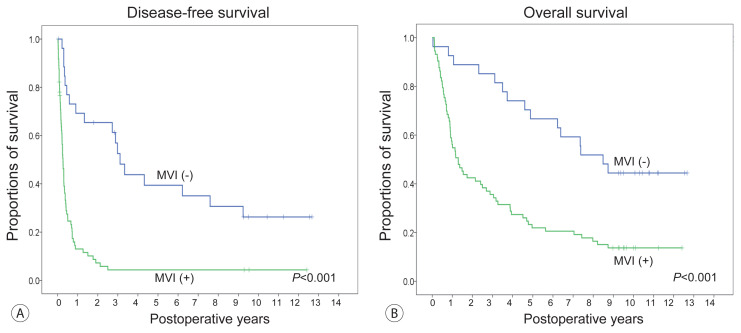
Results: The median tumor diameter and tumor volume were 15.0 cm and 886 mL, respectively. Tumor recurrence and overall survival (OS) rates were 70.7% and 66.0% at one year and 84.9% and 34.0% at five years, respectively. Microvascular invasion (MVI) was the only independent risk factor for disease-free survival (DFS) and OS. DFS and OS, stratified by ADV score with 1-log intervals, showed significant prognostic contrasts (P=0.007 and P=0.017, respectively). DFS and OS, stratified by ADV score with a cut-off of 8-log, showed significant prognostic contrasts (P=0.014 and P=0.042, respectively). The combination of MVI and ADV score with a cut-off of 8-log also showed significant prognostic contrasts in DFS (P<0.001) and OS (P=0.001) considering the number of risk factors. Prognostic contrast was enhanced after combining the MVI and ADV score.
Conclusions: The prognostic prediction model with the ADV score could reliably predict the risk of tumor recurrence and long-term patient survival outcomes in patients with solitary huge HCC ≥13 cm. The results of this study suggest that our prognostic prediction models can be used to guide surgical treatment and post-resection follow-up for patients with huge HCCs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


