Sayed Ali Almahari, Reem Maki, Noor Al Teraifi, Safa Alshaikh, Nisha Chandran, Husain Taha
{"title":"Hashimoto Thyroiditis beyond Cytology: A Correlation between Cytological, Hormonal, Serological, and Radiological Findings.","authors":"Sayed Ali Almahari, Reem Maki, Noor Al Teraifi, Safa Alshaikh, Nisha Chandran, Husain Taha","doi":"10.1155/2023/5707120","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hashimoto thyroiditis is the most common cause of chronic inflammation of the thyroid gland. Ultrasound is the modality for detection, while fine needle aspiration is the gold standard method for diagnosis. Serologic markers, such as antithyroidal peroxidase antibody (TPO) and antithyroglobulin antibody (TG), are usually elevated.</p><p><strong>Aim: </strong>The main objective is to appraise the incidence of neoplasms on a background of Hashimoto thyroiditis. Our second objective is to recognize the different sonographic appearances of Hashimoto thyroiditis, to focus on its nodular and focal patterns, and to measure the sensitivity of the ACR TIRAD system (2017) when interpreted on patients with Hashimoto thyroiditis.</p><p><strong>Methods: </strong>A single-center retrospective cross-sectional study. We studied 137 cases diagnosed cytologically as Hashimoto thyroiditis from January 2013-December 2019. The data collected were analyzed using SPSS (26th edition), and ultrasounds were reviewed by a single board-certified radiologist. The ACR thyroid imaging and Data System 2017 (ACR TI-RADs 2017) and the Bethesda System for reporting thyroid cytology 2017 (BSRTC 2017) were used for reporting ultrasound and cytology, respectively.</p><p><strong>Results: </strong>The mean age was 44.66 years and the female : male was 9 : 1. Serologically, anti-Tg was high in 22 cases (38%), while anti-TPO was positive in all of the 60 cases studied. Histologically, 11 cases were diagnosed with papillary thyroid carcinoma (8%) and a single case with follicular adenoma (0.7%). Ultrasonographically, 50% of the cases showed diffuse pattern, in which 13% of them showed micronodules. 32.2% were macronodular, and 17.7% were a focal nodular pattern. 45 nodules were interpreted with the ACR TIRAD system (2017), in which 22.2% were TR2, 26.6% were TR3, 17.7% were TR4, and 33.3% were TR5.</p><p><strong>Conclusion: </strong>Hashimoto thyroiditis is a risk factor for developing thyroid neoplasms, which necessitate a proper assessment of the cytological material studied and a correlation with the clinical and radiological features. Recognizing the different types of Hashimoto thyroiditis and its variable appearances is significantly important in performing and interpreting thyroid ultrasound imaging. Microcalcification is the most sensitive parameter to discriminate between PTC and nodular type of Hashimoto thyroiditis. The TIRAD system (2017) is a useful tool for risk stratification; however, it might create unnecessary FNA studies in the setting of Hashimoto thyroiditis because of its variable appearances on ultrasound. A modified TIRAD system for patients with Hashimoto thyroiditis is important to alleviate this confusion. Finally, anti-TPO is a sensitive marker for detecting Hashimoto thyroiditis, which could be used for future referencing of newly diagnosed cases.</p>","PeriodicalId":17394,"journal":{"name":"Journal of Thyroid Research","volume":"2023 ","pages":"5707120"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10292943/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/5707120","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction: Hashimoto thyroiditis is the most common cause of chronic inflammation of the thyroid gland. Ultrasound is the modality for detection, while fine needle aspiration is the gold standard method for diagnosis. Serologic markers, such as antithyroidal peroxidase antibody (TPO) and antithyroglobulin antibody (TG), are usually elevated.
Aim: The main objective is to appraise the incidence of neoplasms on a background of Hashimoto thyroiditis. Our second objective is to recognize the different sonographic appearances of Hashimoto thyroiditis, to focus on its nodular and focal patterns, and to measure the sensitivity of the ACR TIRAD system (2017) when interpreted on patients with Hashimoto thyroiditis.
Methods: A single-center retrospective cross-sectional study. We studied 137 cases diagnosed cytologically as Hashimoto thyroiditis from January 2013-December 2019. The data collected were analyzed using SPSS (26th edition), and ultrasounds were reviewed by a single board-certified radiologist. The ACR thyroid imaging and Data System 2017 (ACR TI-RADs 2017) and the Bethesda System for reporting thyroid cytology 2017 (BSRTC 2017) were used for reporting ultrasound and cytology, respectively.
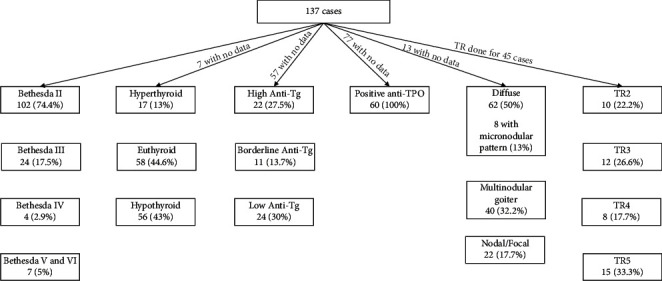
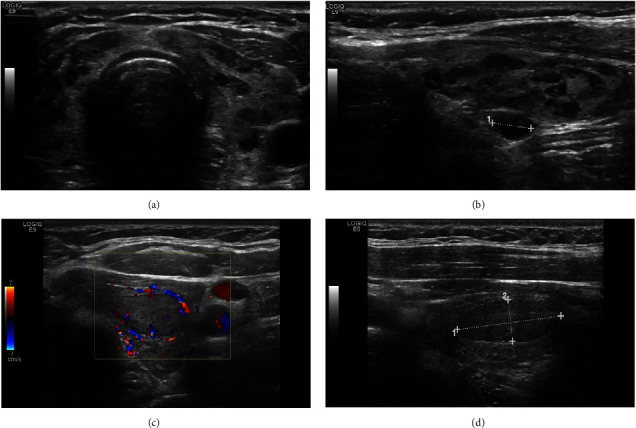
Results: The mean age was 44.66 years and the female : male was 9 : 1. Serologically, anti-Tg was high in 22 cases (38%), while anti-TPO was positive in all of the 60 cases studied. Histologically, 11 cases were diagnosed with papillary thyroid carcinoma (8%) and a single case with follicular adenoma (0.7%). Ultrasonographically, 50% of the cases showed diffuse pattern, in which 13% of them showed micronodules. 32.2% were macronodular, and 17.7% were a focal nodular pattern. 45 nodules were interpreted with the ACR TIRAD system (2017), in which 22.2% were TR2, 26.6% were TR3, 17.7% were TR4, and 33.3% were TR5.
Conclusion: Hashimoto thyroiditis is a risk factor for developing thyroid neoplasms, which necessitate a proper assessment of the cytological material studied and a correlation with the clinical and radiological features. Recognizing the different types of Hashimoto thyroiditis and its variable appearances is significantly important in performing and interpreting thyroid ultrasound imaging. Microcalcification is the most sensitive parameter to discriminate between PTC and nodular type of Hashimoto thyroiditis. The TIRAD system (2017) is a useful tool for risk stratification; however, it might create unnecessary FNA studies in the setting of Hashimoto thyroiditis because of its variable appearances on ultrasound. A modified TIRAD system for patients with Hashimoto thyroiditis is important to alleviate this confusion. Finally, anti-TPO is a sensitive marker for detecting Hashimoto thyroiditis, which could be used for future referencing of newly diagnosed cases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


