{"title":"A cost-effectiveness analysis of COVID-19 critical care interventions in Addis Ababa, Ethiopia: a modeling study.","authors":"Senait Alemayehu Beshah, Arega Zeru, Wogayehu Tadele, Atkure Defar, Theodros Getachew, Lelisa Fekadu Assebe","doi":"10.1186/s12962-023-00446-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To estimate and compare the cost-effectiveness of COVID-19 critical care intervention approaches: noninvasive (oxygen without intubation) and invasive (intubation) management in Ethiopia.</p><p><strong>Methods: </strong>A Markov model is used to compare the costs and outcomes for non-invasive and invasive COVID-19 clinical interventions using both primary and secondary data sources. Healthcare provider costs (recurrent and capital cost) and patient-side costs (direct and indirect) were estimated and reported in United States Dollars (US$), 2021. The outcome measure used in this analysis was DALYs averted. Both the average cost-effectiveness ratio (ACER) and incremental cost-effectiveness ratio (ICER) were reported. One-way and probabilistic sensitivity analyses were applied to assess the robustness of the findings. The analysis is conducted using Tree Age pro health care software 2022.</p><p><strong>Result: </strong>The average cost per patient per episode for mild/moderate, severe, noninvasive, and invasive critical management was $951, $3449, $5514, and $6500, respectively. According to the average cost-effective ratio (ACER), non-invasive management resulted in $1991 per DALY averted, while invasive management resulted in $3998 per DALY averted. Similarly, the incremental cost-effective ratio (ICER) of invasive compared to noninvasive management was $ 4948 per DALY averted.</p><p><strong>Conclusion: </strong>Clinical management of critical COVID-19 cases in Ethiopia is associated with a significant financial burden. Invasive intervention is unlikely to be a cost-effective COVID-19 intervention in Ethiopia compared to noninvasive critical case management using a willingness to pay threshold of three times GDP per capita.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":null,"pages":null},"PeriodicalIF":1.7000,"publicationDate":"2023-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10291773/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-023-00446-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 1
Abstract
Objective: To estimate and compare the cost-effectiveness of COVID-19 critical care intervention approaches: noninvasive (oxygen without intubation) and invasive (intubation) management in Ethiopia.
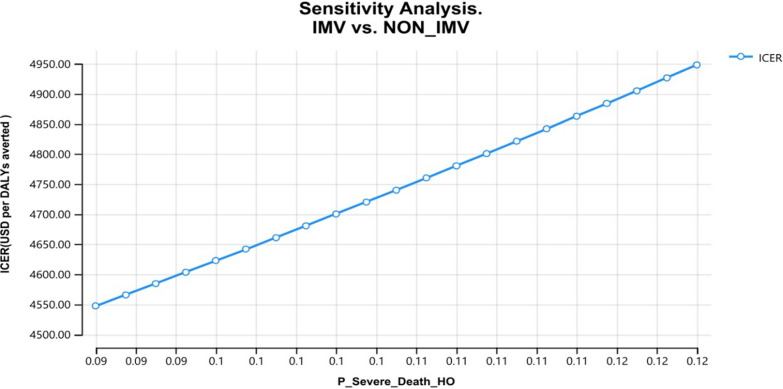
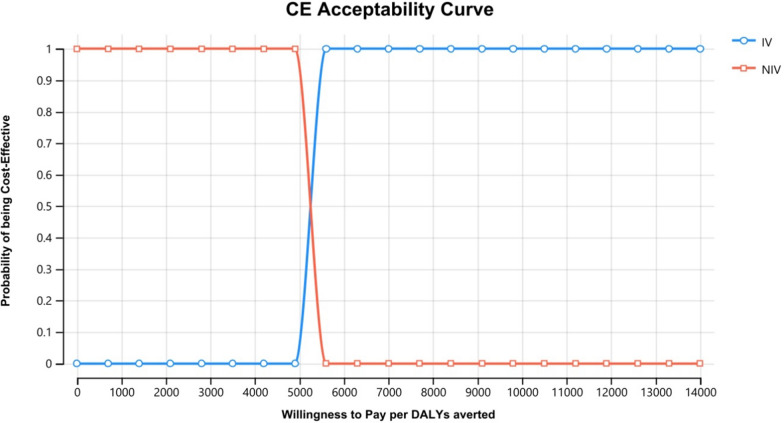
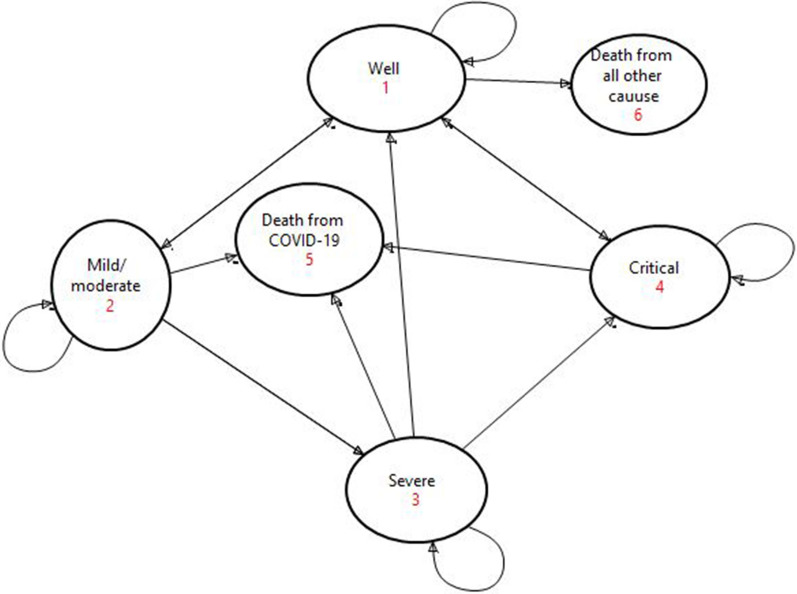
Methods: A Markov model is used to compare the costs and outcomes for non-invasive and invasive COVID-19 clinical interventions using both primary and secondary data sources. Healthcare provider costs (recurrent and capital cost) and patient-side costs (direct and indirect) were estimated and reported in United States Dollars (US$), 2021. The outcome measure used in this analysis was DALYs averted. Both the average cost-effectiveness ratio (ACER) and incremental cost-effectiveness ratio (ICER) were reported. One-way and probabilistic sensitivity analyses were applied to assess the robustness of the findings. The analysis is conducted using Tree Age pro health care software 2022.
Result: The average cost per patient per episode for mild/moderate, severe, noninvasive, and invasive critical management was $951, $3449, $5514, and $6500, respectively. According to the average cost-effective ratio (ACER), non-invasive management resulted in $1991 per DALY averted, while invasive management resulted in $3998 per DALY averted. Similarly, the incremental cost-effective ratio (ICER) of invasive compared to noninvasive management was $ 4948 per DALY averted.
Conclusion: Clinical management of critical COVID-19 cases in Ethiopia is associated with a significant financial burden. Invasive intervention is unlikely to be a cost-effective COVID-19 intervention in Ethiopia compared to noninvasive critical case management using a willingness to pay threshold of three times GDP per capita.
目的:评估和比较埃塞俄比亚COVID-19重症监护干预方法:无创(无氧插管)和有创(插管)管理的成本效益。方法:采用马尔可夫模型比较非侵入性和侵入性COVID-19临床干预的成本和结果。2021年,医疗保健提供者成本(经常性成本和资本成本)和患者成本(直接和间接)以美元(US$)估算和报告。本分析中使用的结局指标是避免DALYs。报告了平均成本-效果比(ACER)和增量成本-效果比(ICER)。应用单向和概率敏感性分析来评估研究结果的稳健性。该分析是使用Tree Age pro保健软件2022进行的。结果:轻/中度、重度、非侵入性和侵入性危重症治疗的每位患者每次发作的平均费用分别为951美元、3449美元、5514美元和6500美元。根据平均成本效益比(ACER),非侵入性管理导致每避免DALY 1991美元,而侵入性管理导致每避免DALY 3998美元。同样,与非侵入性治疗相比,侵入性治疗的增量成本效益比(ICER)为4948美元/每避免DALY。结论:在埃塞俄比亚,COVID-19危重病例的临床管理与重大财政负担相关。在埃塞俄比亚,与使用人均GDP三倍的支付意愿门槛的非侵入性重症病例管理相比,侵入性干预措施不太可能是具有成本效益的COVID-19干预措施。
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


