{"title":"Pseudo-Bartter syndrome in an infant without obvious underlying conditions: A case report.","authors":"Junya Toyoda, Masanori Adachi, Ayako Ochi, Yuki Okada, Aiko Honda, Katsumi Mizuno, Kandai Nozu","doi":"10.1297/cpe.2022-0069","DOIUrl":null,"url":null,"abstract":"<p><p>Pseudo-Bartter syndrome (PBS) develops owing to renal or extrarenal chloride loss, leading to hypokalemic alkalosis. Whereas most adult cases result from diuretic/laxative abuse, many infantile cases occur secondary to cystic fibrosis. Rarely, infantile PBS is caused by renal salt loss with anomalies of the kidney/urinary tract or genetic disorders, such as Dent disease. Here, we report the case of a 10-mo-old girl with a one-month history of decreased formula intake and 5.6% body weight loss. She showed typical laboratory findings as PBS, including hypokalemia (2.7 mEq/L) and high levels of bicarbonate (32.7 mEq/L) with a plasma renin activity of 399 ng/mL/h. With minimum supplementation of potassium and sodium, an improvement in body mass index, from -1.13 SD to +0.52 SD, with complete resolution of laboratory data was obtained in approximately one month. No causative mutations were identified in candidate genes for Bartter-Gitelman syndrome. Due to profound hypochloruria (< 15 mEq/L), PBS of renal origin was unlikely. In addition, extrarenal chloride loss did not seem to be the case, because the patient never manifested gastrointestinal symptoms. Therefore, we speculate that a temporary decrease in chloride intake, coupled with the putative genetic/epigenetic disadvantage of chloride retention, such as a subtle renal leak, may be responsible for the PBS in our patient.</p>","PeriodicalId":10678,"journal":{"name":"Clinical Pediatric Endocrinology","volume":null,"pages":null},"PeriodicalIF":1.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/02/cpe-32-155.PMC10288294.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pediatric Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1297/cpe.2022-0069","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
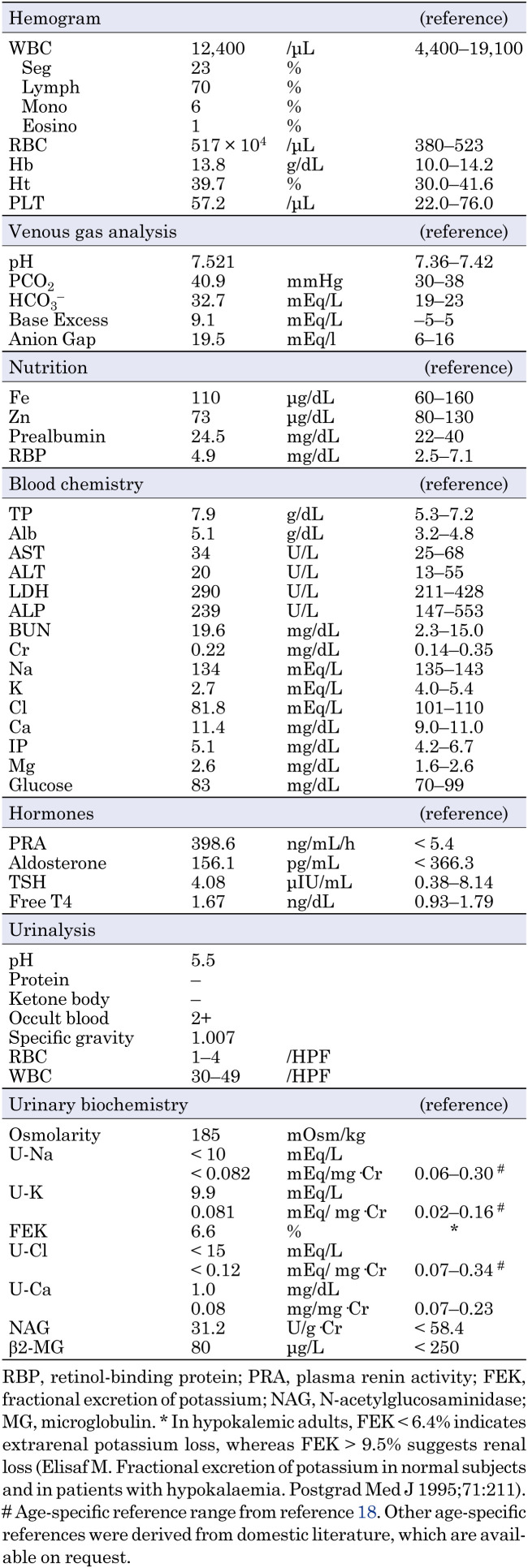
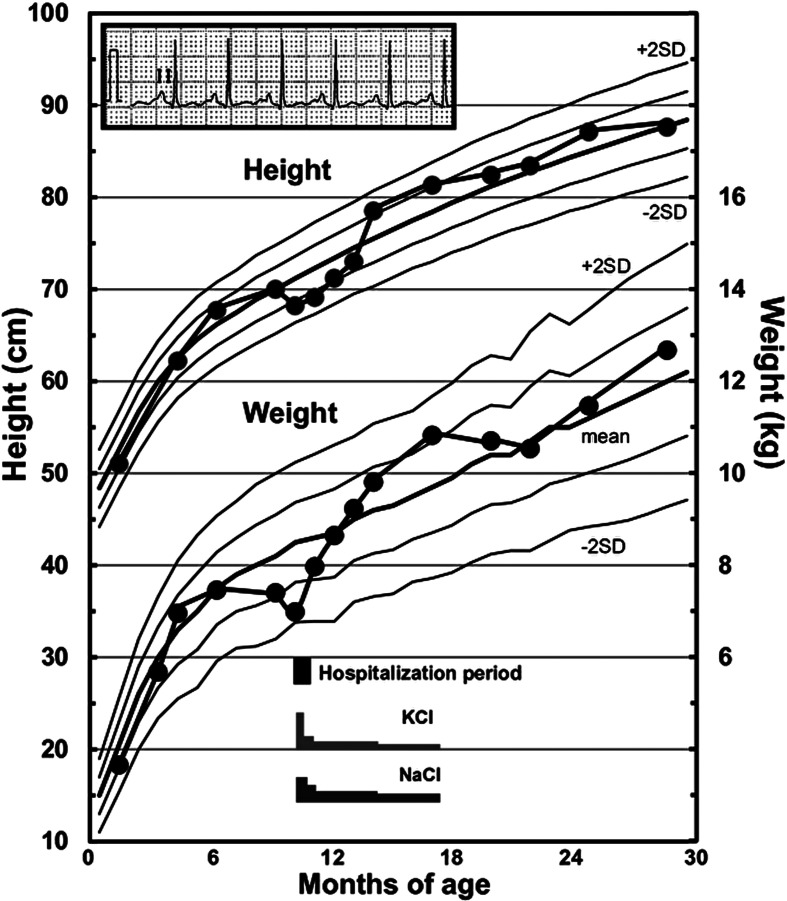
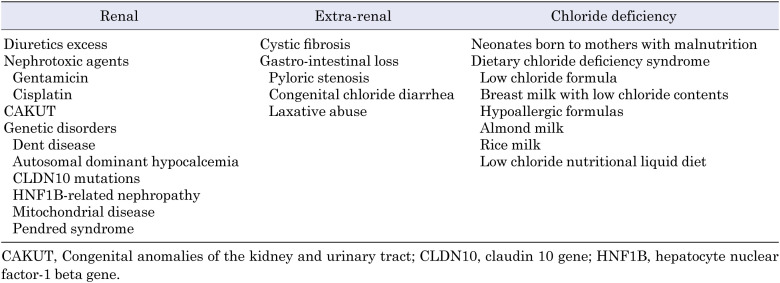
Pseudo-Bartter syndrome (PBS) develops owing to renal or extrarenal chloride loss, leading to hypokalemic alkalosis. Whereas most adult cases result from diuretic/laxative abuse, many infantile cases occur secondary to cystic fibrosis. Rarely, infantile PBS is caused by renal salt loss with anomalies of the kidney/urinary tract or genetic disorders, such as Dent disease. Here, we report the case of a 10-mo-old girl with a one-month history of decreased formula intake and 5.6% body weight loss. She showed typical laboratory findings as PBS, including hypokalemia (2.7 mEq/L) and high levels of bicarbonate (32.7 mEq/L) with a plasma renin activity of 399 ng/mL/h. With minimum supplementation of potassium and sodium, an improvement in body mass index, from -1.13 SD to +0.52 SD, with complete resolution of laboratory data was obtained in approximately one month. No causative mutations were identified in candidate genes for Bartter-Gitelman syndrome. Due to profound hypochloruria (< 15 mEq/L), PBS of renal origin was unlikely. In addition, extrarenal chloride loss did not seem to be the case, because the patient never manifested gastrointestinal symptoms. Therefore, we speculate that a temporary decrease in chloride intake, coupled with the putative genetic/epigenetic disadvantage of chloride retention, such as a subtle renal leak, may be responsible for the PBS in our patient.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


