Björn Stessel, Maayeen Bin Saad, Lotte Ullrick, Laurien Geebelen, Jeroen Lehaen, Philippe Jr Timmermans, Michiel Van Tornout, Ina Callebaut, Jeroen Vandenbrande, Jasperina Dubois
{"title":"Extracorporeal Membrane Oxygenation to Support COVID-19 Patients: A Propensity-Matched Cohort Study.","authors":"Björn Stessel, Maayeen Bin Saad, Lotte Ullrick, Laurien Geebelen, Jeroen Lehaen, Philippe Jr Timmermans, Michiel Van Tornout, Ina Callebaut, Jeroen Vandenbrande, Jasperina Dubois","doi":"10.1155/2023/5101456","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with severe respiratory failure from COVID-19, extracorporeal membrane oxygenation (ECMO) treatment can facilitate lung-protective ventilation and may improve outcome and survival if conventional therapy fails to assure adequate oxygenation and ventilation. We aimed to perform a confirmatory propensity-matched cohort study comparing the impact of ECMO and maximum invasive mechanical ventilation alone (MVA) on mortality and complications in severe COVID-19 pneumonia.</p><p><strong>Materials and methods: </strong>All 295 consecutive adult patients with confirmed COVID-19 pneumonia admitted to the intensive care unit (ICU) from March 13<sup>th</sup>, 2020, to July 31<sup>st</sup>, 2021 were included. At admission, all patients were classified into 3 categories: (1) full code including the initiation of ECMO therapy (AAA code), (2) full code excluding ECMO (AA code), and (3) do-not-intubate (A code). For the 271 non-ECMO patients, match eligibility was determined for all patients with the AAA code treated with MVA. Propensity score matching was performed using a logistic regression model including the following variables: gender, P/F ratio, SOFA score at admission, and date of ICU admission. The primary endpoint was ICU mortality.</p><p><strong>Results: </strong>A total of 24 ECMO patients were propensity matched to an equal number of MVA patients. ICU mortality was significantly higher in the ECMO arm (45.8%) compared with the MVA cohort (16.67%) (OR 4.23 (1.11, 16.17); <i>p</i>=0.02). Three-month mortality was 50% with ECMO compared to 16.67% after MVA (OR 5.91 (1.55, 22.58); <i>p</i> < 0.01). Applied peak inspiratory pressures (33.42 ± 8.52 vs. 24.74 ± 4.86 mmHg; <i>p</i> < 0.01) and maximal PEEP levels (14.47 ± 3.22 vs. 13.52 ± 3.86 mmHg; <i>p</i>=0.01) were higher with MVA. ICU length of stay (LOS) and hospital LOS were comparable in both groups.</p><p><strong>Conclusion: </strong>ECMO therapy may be associated with an up to a three-fold increase in ICU mortality and 3-month mortality compared to MVA despite the facilitation of lung-protective ventilation settings in mechanically ventilated COVID-19 patients. We cannot confirm the positive results of the first propensity-matched cohort study on this topic. This trial is registered with NCT05158816.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2023 ","pages":"5101456"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10279486/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/5101456","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In patients with severe respiratory failure from COVID-19, extracorporeal membrane oxygenation (ECMO) treatment can facilitate lung-protective ventilation and may improve outcome and survival if conventional therapy fails to assure adequate oxygenation and ventilation. We aimed to perform a confirmatory propensity-matched cohort study comparing the impact of ECMO and maximum invasive mechanical ventilation alone (MVA) on mortality and complications in severe COVID-19 pneumonia.
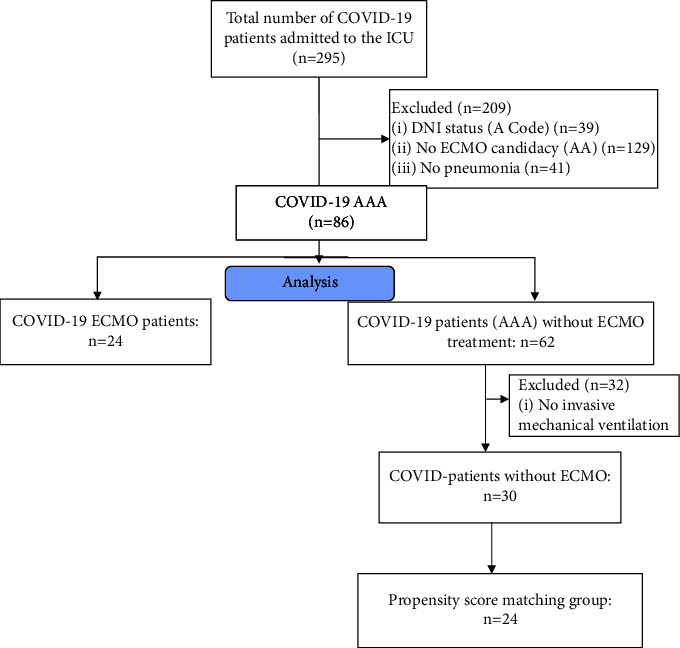
Materials and methods: All 295 consecutive adult patients with confirmed COVID-19 pneumonia admitted to the intensive care unit (ICU) from March 13th, 2020, to July 31st, 2021 were included. At admission, all patients were classified into 3 categories: (1) full code including the initiation of ECMO therapy (AAA code), (2) full code excluding ECMO (AA code), and (3) do-not-intubate (A code). For the 271 non-ECMO patients, match eligibility was determined for all patients with the AAA code treated with MVA. Propensity score matching was performed using a logistic regression model including the following variables: gender, P/F ratio, SOFA score at admission, and date of ICU admission. The primary endpoint was ICU mortality.
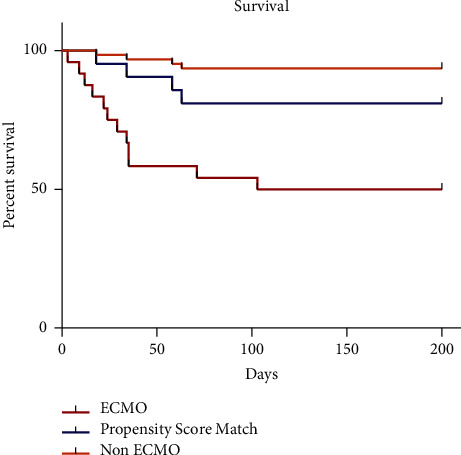
Results: A total of 24 ECMO patients were propensity matched to an equal number of MVA patients. ICU mortality was significantly higher in the ECMO arm (45.8%) compared with the MVA cohort (16.67%) (OR 4.23 (1.11, 16.17); p=0.02). Three-month mortality was 50% with ECMO compared to 16.67% after MVA (OR 5.91 (1.55, 22.58); p < 0.01). Applied peak inspiratory pressures (33.42 ± 8.52 vs. 24.74 ± 4.86 mmHg; p < 0.01) and maximal PEEP levels (14.47 ± 3.22 vs. 13.52 ± 3.86 mmHg; p=0.01) were higher with MVA. ICU length of stay (LOS) and hospital LOS were comparable in both groups.
Conclusion: ECMO therapy may be associated with an up to a three-fold increase in ICU mortality and 3-month mortality compared to MVA despite the facilitation of lung-protective ventilation settings in mechanically ventilated COVID-19 patients. We cannot confirm the positive results of the first propensity-matched cohort study on this topic. This trial is registered with NCT05158816.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


