{"title":"Treatment strategy for children and adolescents with type 2 diabetes-based on ISPAD Clinical Practice Consensus Guidelines 2022.","authors":"Tatsuhiko Urakami","doi":"10.1297/cpe.2023-0007","DOIUrl":null,"url":null,"abstract":"<p><p>The principles of treatment for children and adolescents with type 2 diabetes include dietary and exercise management. For dietary management, a relatively modest dietary regimen with an appropriate energy source composition is recommended. Moderate- to vigorous-intensity aerobic activity is recommended for at least 60 min/d. Family members are encouraged to modify their lifestyles. Some patients fail to improve hyperglycemia through dietary and exercise management and eventually require pharmacological treatment. If the patient is metabolically stable (HbA1c level < 8.5% [69 mmol/mol]), metformin is the first-line treatment of first choice. In a case with ketosis or HbA1c of more than 8.5% (69 mmol/mol), insulin will be required initially with once daily basal insulin (0.25-0.5 units/kg). The goal of the initial treatment is to attain an HbA1c level < 7.0% (53 mmol/mol). If the glycemic goal is not attained, the addition of a second agent should be considered. However, the use of antihyperglycemic drugs in pediatric patients is limited in most countries. Therefore, the efficacy and safety of these drugs used in adult patients, including GLP-1 receptor agonists and SGLT2 inhibitors, should be evaluated in pediatric patients worldwide.</p>","PeriodicalId":10678,"journal":{"name":"Clinical Pediatric Endocrinology","volume":null,"pages":null},"PeriodicalIF":1.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/76/e2/cpe-32-125.PMC10288292.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pediatric Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1297/cpe.2023-0007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/21 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
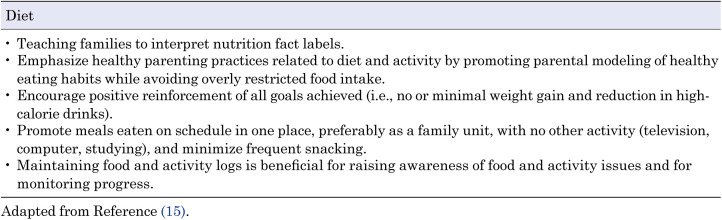
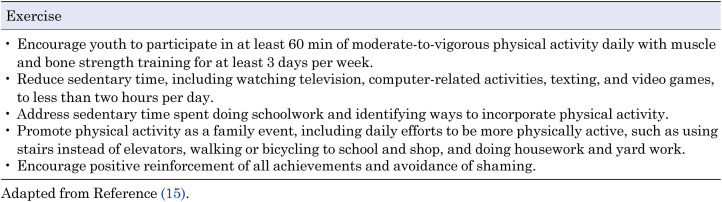
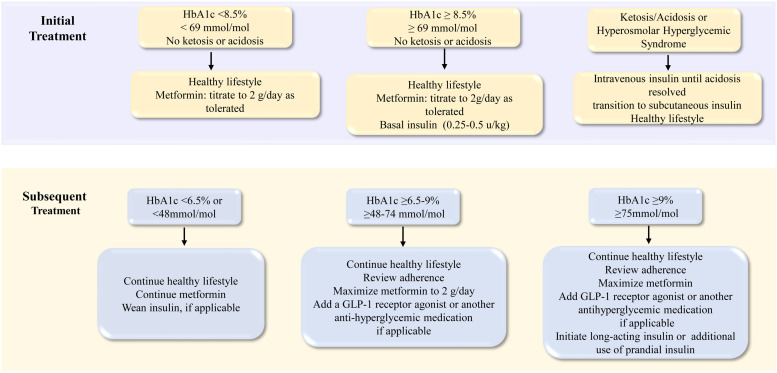
The principles of treatment for children and adolescents with type 2 diabetes include dietary and exercise management. For dietary management, a relatively modest dietary regimen with an appropriate energy source composition is recommended. Moderate- to vigorous-intensity aerobic activity is recommended for at least 60 min/d. Family members are encouraged to modify their lifestyles. Some patients fail to improve hyperglycemia through dietary and exercise management and eventually require pharmacological treatment. If the patient is metabolically stable (HbA1c level < 8.5% [69 mmol/mol]), metformin is the first-line treatment of first choice. In a case with ketosis or HbA1c of more than 8.5% (69 mmol/mol), insulin will be required initially with once daily basal insulin (0.25-0.5 units/kg). The goal of the initial treatment is to attain an HbA1c level < 7.0% (53 mmol/mol). If the glycemic goal is not attained, the addition of a second agent should be considered. However, the use of antihyperglycemic drugs in pediatric patients is limited in most countries. Therefore, the efficacy and safety of these drugs used in adult patients, including GLP-1 receptor agonists and SGLT2 inhibitors, should be evaluated in pediatric patients worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


