Impact of a Prior Cancer Diagnosis on Quality of Care and Survival Following Acute Myocardial Infarction: Retrospective Population-Based Cohort Study in England.
Lucy Teece, Michael J Sweeting, Marlous Hall, Briana Coles, Clare Oliver-Williams, Cathy A Welch, Mark A de Belder, John Deanfield, Clive Weston, Mark J Rutherford, Lizz Paley, Umesh T Kadam, Paul C Lambert, Michael D Peake, Chris P Gale, David Adlam
{"title":"Impact of a Prior Cancer Diagnosis on Quality of Care and Survival Following Acute Myocardial Infarction: Retrospective Population-Based Cohort Study in England.","authors":"Lucy Teece, Michael J Sweeting, Marlous Hall, Briana Coles, Clare Oliver-Williams, Cathy A Welch, Mark A de Belder, John Deanfield, Clive Weston, Mark J Rutherford, Lizz Paley, Umesh T Kadam, Paul C Lambert, Michael D Peake, Chris P Gale, David Adlam","doi":"10.1161/CIRCOUTCOMES.122.009236","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>An increasing proportion of patients with cancer experience acute myocardial infarction (AMI). We investigated differences in quality of AMI care and survival between patients with and without previous cancer diagnoses.</p><p><strong>Methods: </strong>A retrospective cohort study using Virtual Cardio-Oncology Research Initiative data. Patients aged 40+ years hospitalized in England with AMI between January 2010 and March 2018 were assessed, ascertaining previous cancers diagnosed within 15 years. Multivariable regression was used to assess effects of cancer diagnosis, time, stage, and site on international quality indicators and mortality.</p><p><strong>Results: </strong>Of 512 388 patients with AMI (mean age, 69.3 years; 33.5% women), 42 187 (8.2%) had previous cancers. Patients with cancer had significantly lower use of ACE (angiotensin-converting enzyme) inhibitors/angiotensin receptor blockers (mean percentage point decrease [mppd], 2.6% [95% CI, 1.8-3.4]) and lower overall composite care (mppd, 1.2% [95% CI, 0.9-1.6]). Poorer quality indicator attainment was observed in patients with cancer diagnosed in the last year (mppd, 1.4% [95% CI, 1.8-1.0]), with later stage disease (mppd, 2.5% [95% CI, 3.3-1.4]), and with lung cancer (mppd, 2.2% [95% CI, 3.0-1.3]). Twelve-month all-cause survival was 90.5% in noncancer controls and 86.3% in adjusted counterfactual controls. Differences in post-AMI survival were driven by cancer-related deaths. Modeling improving quality indicator attainment to noncancer patient levels showed modest 12-month survival benefits (lung cancer, 0.6%; other cancers, 0.3%).</p><p><strong>Conclusions: </strong>Measures of quality of AMI care are poorer in patients with cancer, with lower use of secondary prevention medications. Findings are primarily driven by differences in age and comorbidities between cancer and noncancer populations and attenuated after adjustment. The largest impact was observed in recent cancer diagnoses (<1 year) and lung cancer. Further investigation will determine whether differences reflect appropriate management according to cancer prognosis or whether opportunities to improve AMI outcomes in patients with cancer exist.</p>","PeriodicalId":10301,"journal":{"name":"Circulation. Cardiovascular Quality and Outcomes","volume":"16 6","pages":"e009236"},"PeriodicalIF":6.7000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10281182/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation. Cardiovascular Quality and Outcomes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1161/CIRCOUTCOMES.122.009236","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/20 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: An increasing proportion of patients with cancer experience acute myocardial infarction (AMI). We investigated differences in quality of AMI care and survival between patients with and without previous cancer diagnoses.
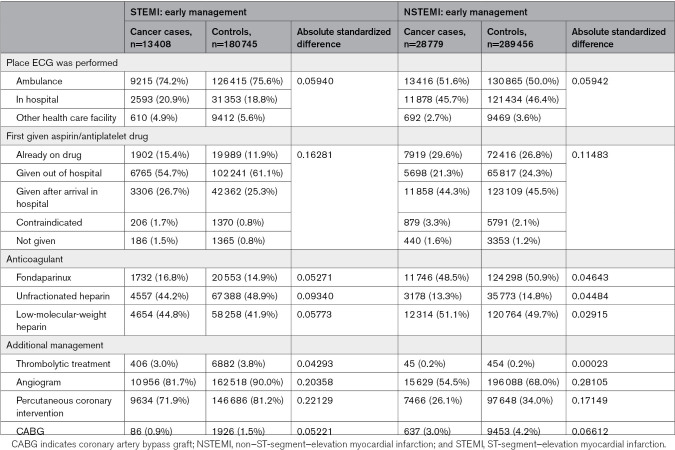
Methods: A retrospective cohort study using Virtual Cardio-Oncology Research Initiative data. Patients aged 40+ years hospitalized in England with AMI between January 2010 and March 2018 were assessed, ascertaining previous cancers diagnosed within 15 years. Multivariable regression was used to assess effects of cancer diagnosis, time, stage, and site on international quality indicators and mortality.
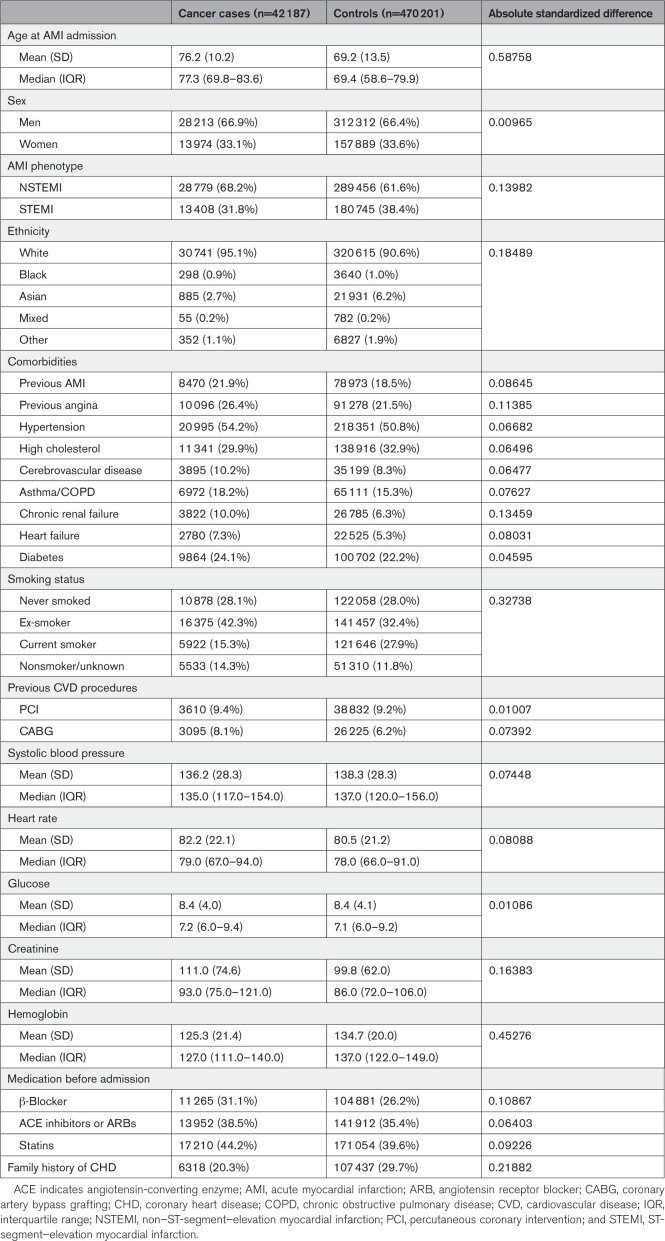
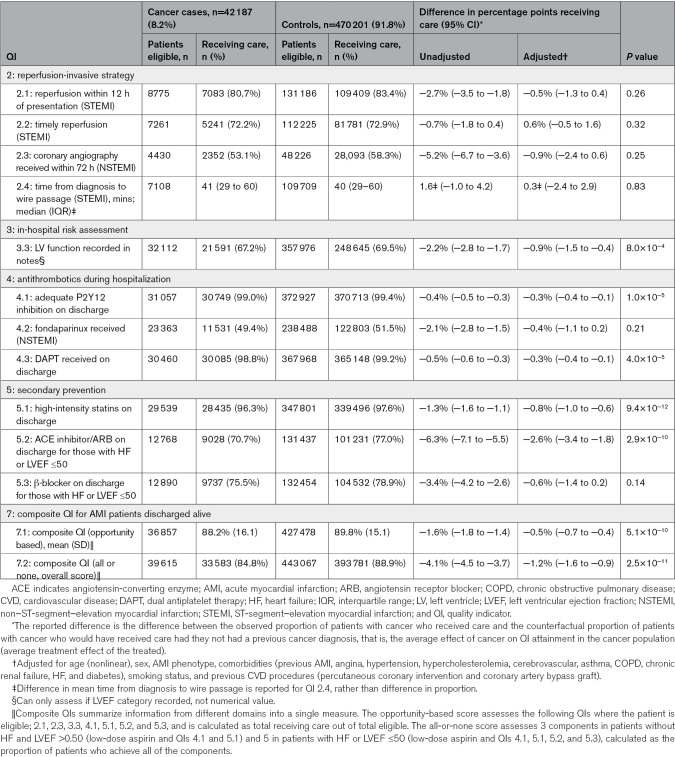
Results: Of 512 388 patients with AMI (mean age, 69.3 years; 33.5% women), 42 187 (8.2%) had previous cancers. Patients with cancer had significantly lower use of ACE (angiotensin-converting enzyme) inhibitors/angiotensin receptor blockers (mean percentage point decrease [mppd], 2.6% [95% CI, 1.8-3.4]) and lower overall composite care (mppd, 1.2% [95% CI, 0.9-1.6]). Poorer quality indicator attainment was observed in patients with cancer diagnosed in the last year (mppd, 1.4% [95% CI, 1.8-1.0]), with later stage disease (mppd, 2.5% [95% CI, 3.3-1.4]), and with lung cancer (mppd, 2.2% [95% CI, 3.0-1.3]). Twelve-month all-cause survival was 90.5% in noncancer controls and 86.3% in adjusted counterfactual controls. Differences in post-AMI survival were driven by cancer-related deaths. Modeling improving quality indicator attainment to noncancer patient levels showed modest 12-month survival benefits (lung cancer, 0.6%; other cancers, 0.3%).
Conclusions: Measures of quality of AMI care are poorer in patients with cancer, with lower use of secondary prevention medications. Findings are primarily driven by differences in age and comorbidities between cancer and noncancer populations and attenuated after adjustment. The largest impact was observed in recent cancer diagnoses (<1 year) and lung cancer. Further investigation will determine whether differences reflect appropriate management according to cancer prognosis or whether opportunities to improve AMI outcomes in patients with cancer exist.
期刊介绍:
Circulation: Cardiovascular Quality and Outcomes, an American Heart Association journal, publishes articles related to improving cardiovascular health and health care. Content includes original research, reviews, and case studies relevant to clinical decision-making and healthcare policy. The online-only journal is dedicated to furthering the mission of promoting safe, effective, efficient, equitable, timely, and patient-centered care. Through its articles and contributions, the journal equips you with the knowledge you need to improve clinical care and population health, and allows you to engage in scholarly activities of consequence to the health of the public. Circulation: Cardiovascular Quality and Outcomes considers the following types of articles: Original Research Articles, Data Reports, Methods Papers, Cardiovascular Perspectives, Care Innovations, Novel Statistical Methods, Policy Briefs, Data Visualizations, and Caregiver or Patient Viewpoints.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


