{"title":"Extent of Lymph Node Dissection in Patients with Small-Sized Peripheral Non-Small Cell Lung Cancer during Intentional Segmentectomy.","authors":"Tomohiro Maniwa, Masayuki Ohue, Yasushi Shintani, Jiro Okami","doi":"10.5761/atcs.oa.22-00216","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Segmentectomy and mediastinal lymph node dissection (MLND) are becoming standard procedures for small-sized (<2 cm) peripheral non-small cell lung cancer (NSCLC). Although the benefits of the less resected lung are proven, the extent of lymph node dissection remains unchanged.</p><p><strong>Methods: </strong>We studied 422 patients who underwent lobectomy with MLND (lobe specific or systemic) for small peripheral NSCLC with clinical N0 disease. Patients with middle lobectomy (n = 39) and a consolidation-to-tumor (C/T) ratio ≤0.50 (n = 33) were excluded. We investigated the clinical factors, lymph node metastasis distributions, and lymph node recurrence patterns of 350 patients.</p><p><strong>Results: </strong>Thirty-five (10.0%) patients had lymph node metastasis; none with C/T ratio <0.75 had lymph node metastasis and lymph node recurrence. None had solitary lymph node metastasis in the outside lobe-specific MLND. Six patients had mediastinal lymph node metastasis at the initial site of recurrence; none had mediastinal lymph node recurrence outside the lobe-specific MLND, except for two patients with S6 primary disease.</p><p><strong>Conclusion: </strong>NSCLC patients with small peripheral tumors and a C/T ratio <0.75 during segmentectomy may not require MLND. The optimal MLND for patients with a C/T ratio ≥0.75, except for those with S6 primary, may be lobe-specific MLND.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":" ","pages":"271-278"},"PeriodicalIF":1.3000,"publicationDate":"2023-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10767659/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.22-00216","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/25 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: Segmentectomy and mediastinal lymph node dissection (MLND) are becoming standard procedures for small-sized (<2 cm) peripheral non-small cell lung cancer (NSCLC). Although the benefits of the less resected lung are proven, the extent of lymph node dissection remains unchanged.
Methods: We studied 422 patients who underwent lobectomy with MLND (lobe specific or systemic) for small peripheral NSCLC with clinical N0 disease. Patients with middle lobectomy (n = 39) and a consolidation-to-tumor (C/T) ratio ≤0.50 (n = 33) were excluded. We investigated the clinical factors, lymph node metastasis distributions, and lymph node recurrence patterns of 350 patients.
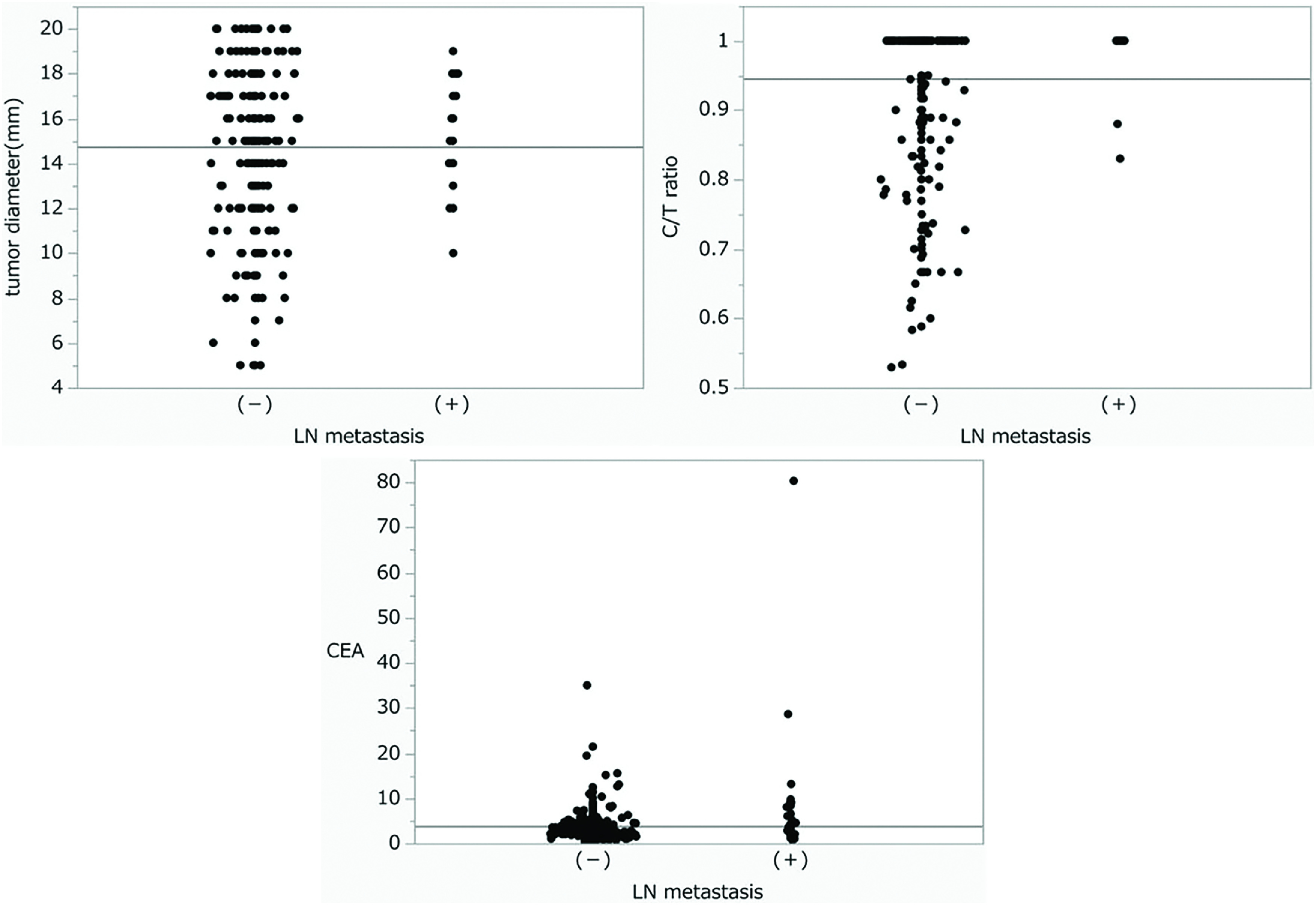
Results: Thirty-five (10.0%) patients had lymph node metastasis; none with C/T ratio <0.75 had lymph node metastasis and lymph node recurrence. None had solitary lymph node metastasis in the outside lobe-specific MLND. Six patients had mediastinal lymph node metastasis at the initial site of recurrence; none had mediastinal lymph node recurrence outside the lobe-specific MLND, except for two patients with S6 primary disease.
Conclusion: NSCLC patients with small peripheral tumors and a C/T ratio <0.75 during segmentectomy may not require MLND. The optimal MLND for patients with a C/T ratio ≥0.75, except for those with S6 primary, may be lobe-specific MLND.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


