Rebecca A Dennison, Lily C Taylor, Stephen Morris, Rachel A Boscott, Hannah Harrison, Sowmiya A Moorthie, Sabrina H Rossi, Grant D Stewart, Juliet A Usher-Smith
{"title":"Public Preferences for Determining Eligibility for Screening in Risk-Stratified Cancer Screening Programs: A Discrete Choice Experiment.","authors":"Rebecca A Dennison, Lily C Taylor, Stephen Morris, Rachel A Boscott, Hannah Harrison, Sowmiya A Moorthie, Sabrina H Rossi, Grant D Stewart, Juliet A Usher-Smith","doi":"10.1177/0272989X231155790","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Risk stratification has been proposed to improve the efficiency of population-level cancer screening. We aimed to describe and quantify the relative importance of different attributes of potential screening programs among the public, focusing on stratifying eligibility.</p><p><strong>Methods: </strong>We conducted a discrete choice experiment in which respondents selected between 2 hypothetical screening programs in a series of 9 questions. We presented the risk factors used to determine eligibility (age, sex, or lifestyle or genetic risk scores) and anticipated outcomes based on eligibility criteria with different sensitivity and specificity levels. We performed conditional logit regression models and used the results to estimate preferences for different approaches. We also analyzed free-text comments on respondents' views on the programs.</p><p><strong>Results: </strong>A total of 1,172 respondents completed the survey. Sensitivity was the most important attribute (7 and 11 times more important than specificity and risk factors, respectively). Eligibility criteria based on age and sex or genetics were preferred over age alone and lifestyle risk scores. Phenotypic and polygenic risk prediction models would be more acceptable than screening everyone aged 55 to 70 y if they had high discrimination (area under the receiver-operating characteristic curve ≥0.75 and 0.80, respectively).</p><p><strong>Limitations: </strong>Although our sample was representative with respect to age, sex, and ethnicity, it may not be representative of the UK population regarding other important characteristics. Also, some respondents may have not understood all the information provided to inform decision making.</p><p><strong>Conclusions: </strong>The public prioritized lives saved from cancer over reductions in numbers screened or experiencing unnecessary follow-up. Incorporating personal-level risk factors into screening eligibility criteria is acceptable to the public if it increases sensitivity; therefore, maximizing sensitivity in model development and communication could increase uptake.</p><p><strong>Highlights: </strong>The public prioritized lives saved when considering changing from age-based eligibility criteria to risk-stratified cancer screening over reductions in numbers of people being screened or experiencing unnecessary follow-up.The risk stratification strategy used to do this was the least important component, although age plus sex or genetics were relatively preferable to using age alone and lifestyle risk scores.Communication strategies that emphasize improvements in the numbers of cancers detected or not missed across the population are more likely to be salient than reductions in unnecessary investigations or follow-up among some groups.Future research should focus on developing implementation strategies that maximize gains in sensitivity within the context of resource constraints and how to present attributes relating to specificity to facilitate understanding and informed decision making.</p>","PeriodicalId":49839,"journal":{"name":"Medical Decision Making","volume":"43 3","pages":"374-386"},"PeriodicalIF":3.1000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10021112/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Decision Making","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/0272989X231155790","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Risk stratification has been proposed to improve the efficiency of population-level cancer screening. We aimed to describe and quantify the relative importance of different attributes of potential screening programs among the public, focusing on stratifying eligibility.
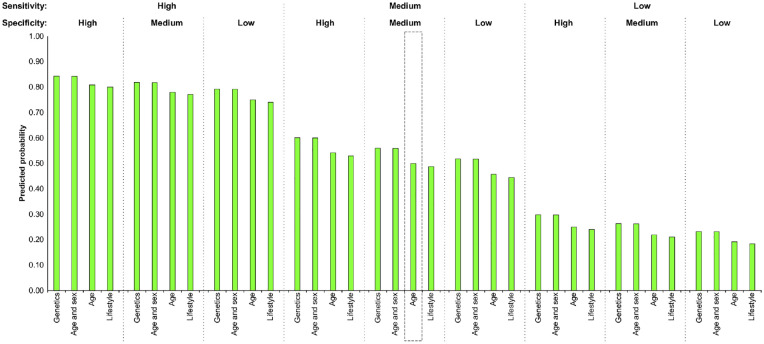
Methods: We conducted a discrete choice experiment in which respondents selected between 2 hypothetical screening programs in a series of 9 questions. We presented the risk factors used to determine eligibility (age, sex, or lifestyle or genetic risk scores) and anticipated outcomes based on eligibility criteria with different sensitivity and specificity levels. We performed conditional logit regression models and used the results to estimate preferences for different approaches. We also analyzed free-text comments on respondents' views on the programs.
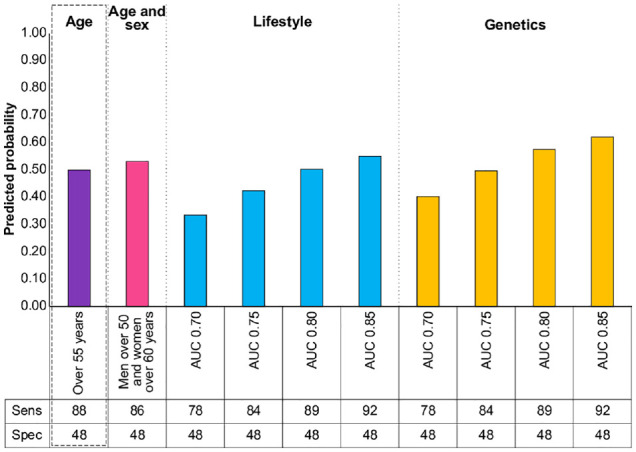
Results: A total of 1,172 respondents completed the survey. Sensitivity was the most important attribute (7 and 11 times more important than specificity and risk factors, respectively). Eligibility criteria based on age and sex or genetics were preferred over age alone and lifestyle risk scores. Phenotypic and polygenic risk prediction models would be more acceptable than screening everyone aged 55 to 70 y if they had high discrimination (area under the receiver-operating characteristic curve ≥0.75 and 0.80, respectively).
Limitations: Although our sample was representative with respect to age, sex, and ethnicity, it may not be representative of the UK population regarding other important characteristics. Also, some respondents may have not understood all the information provided to inform decision making.
Conclusions: The public prioritized lives saved from cancer over reductions in numbers screened or experiencing unnecessary follow-up. Incorporating personal-level risk factors into screening eligibility criteria is acceptable to the public if it increases sensitivity; therefore, maximizing sensitivity in model development and communication could increase uptake.
Highlights: The public prioritized lives saved when considering changing from age-based eligibility criteria to risk-stratified cancer screening over reductions in numbers of people being screened or experiencing unnecessary follow-up.The risk stratification strategy used to do this was the least important component, although age plus sex or genetics were relatively preferable to using age alone and lifestyle risk scores.Communication strategies that emphasize improvements in the numbers of cancers detected or not missed across the population are more likely to be salient than reductions in unnecessary investigations or follow-up among some groups.Future research should focus on developing implementation strategies that maximize gains in sensitivity within the context of resource constraints and how to present attributes relating to specificity to facilitate understanding and informed decision making.
期刊介绍:
Medical Decision Making offers rigorous and systematic approaches to decision making that are designed to improve the health and clinical care of individuals and to assist with health care policy development. Using the fundamentals of decision analysis and theory, economic evaluation, and evidence based quality assessment, Medical Decision Making presents both theoretical and practical statistical and modeling techniques and methods from a variety of disciplines.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


