Turki B Albacker, Amr A Arafat, Abdulaziz M Alotaibi, Haneen Alghosoon, Khalid D Algarni
{"title":"Mechanical Tricuspid Valves Have Higher Rate of Reintervention: A Single Center Experience.","authors":"Turki B Albacker, Amr A Arafat, Abdulaziz M Alotaibi, Haneen Alghosoon, Khalid D Algarni","doi":"10.5761/atcs.oa.22-00086","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We compared the composite outcome of tricuspid valve (TV) reintervention or heart failure (HF) admission in patients who underwent tricuspid valve replacement (TVR) with tissue vs. mechanical valves.</p><p><strong>Patients and methods: </strong>The study included 159 patients who underwent TVR from 2009 to 2019. We grouped the patients according to the valve's type into tissue valve group (n = 139) and mechanical valve group (n = 20).</p><p><strong>Results: </strong>The mean age of patients was 52.4 ± 12.8 years, and 117 patients were females (73.6%). Hospital mortality occurred in 20 patients (12.6%); all of them were in the tissue valve group. The composite outcome of reintervention and HF readmission occurred in 8 patients with mechanical valves (40%) vs. 24 patients with tissue valves (17.3%), (P = 0.018). Predictors of reintervention and HF admission were female (subdistributional hazard ratio [SHR]: 1.38-34.3, P = 0.019), stroke (SHR: 1.25-8.76, P = 0.016), hypertension (SHR: 1.13-5.36, P = 0.024), and mechanical valves (SHR: 1.6-10.7, P = 0.003). In post hoc analysis, the difference in the composite outcome was derived from the difference in the reintervention rate that was higher in mechanical valves. Survival did not differ significantly between groups (P = 0.12).</p><p><strong>Conclusion: </strong>Mechanical TVs have a higher rate of composite outcome of reintervention or HF readmission than tissue TVs that are related mainly to higher rate of reintervention.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"29 2","pages":"78-85"},"PeriodicalIF":1.3000,"publicationDate":"2023-04-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d3/46/atcs-29-078.PMC10126767.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.22-00086","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 2
Abstract
Purpose: We compared the composite outcome of tricuspid valve (TV) reintervention or heart failure (HF) admission in patients who underwent tricuspid valve replacement (TVR) with tissue vs. mechanical valves.
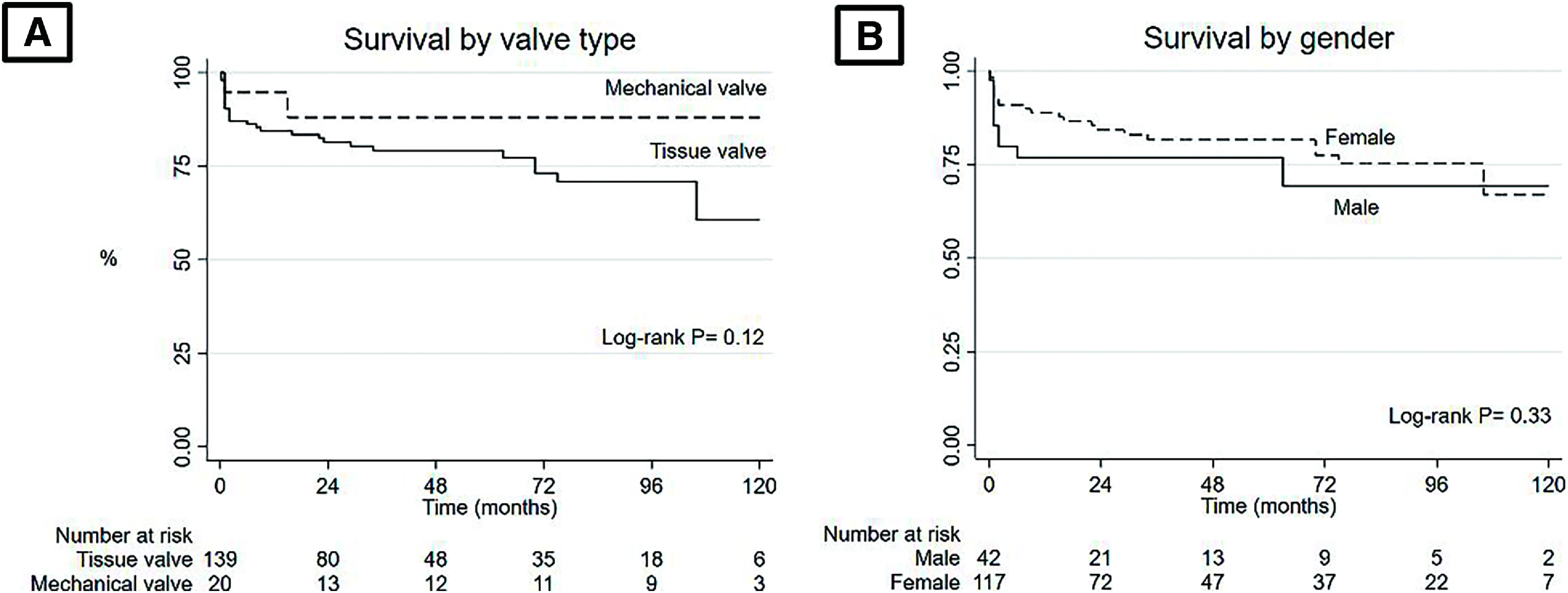
Patients and methods: The study included 159 patients who underwent TVR from 2009 to 2019. We grouped the patients according to the valve's type into tissue valve group (n = 139) and mechanical valve group (n = 20).
Results: The mean age of patients was 52.4 ± 12.8 years, and 117 patients were females (73.6%). Hospital mortality occurred in 20 patients (12.6%); all of them were in the tissue valve group. The composite outcome of reintervention and HF readmission occurred in 8 patients with mechanical valves (40%) vs. 24 patients with tissue valves (17.3%), (P = 0.018). Predictors of reintervention and HF admission were female (subdistributional hazard ratio [SHR]: 1.38-34.3, P = 0.019), stroke (SHR: 1.25-8.76, P = 0.016), hypertension (SHR: 1.13-5.36, P = 0.024), and mechanical valves (SHR: 1.6-10.7, P = 0.003). In post hoc analysis, the difference in the composite outcome was derived from the difference in the reintervention rate that was higher in mechanical valves. Survival did not differ significantly between groups (P = 0.12).
Conclusion: Mechanical TVs have a higher rate of composite outcome of reintervention or HF readmission than tissue TVs that are related mainly to higher rate of reintervention.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


