Young Un Choi, Jun Gi Kim, Ji Young Jang, Tae Hwa Go, Kwangmin Kim, Keum Seok Bae, Hongjin Shim
{"title":"Adjuvant intravenous immunoglobulin administration on postoperative critically ill patients with secondary peritonitis: a retrospective study.","authors":"Young Un Choi, Jun Gi Kim, Ji Young Jang, Tae Hwa Go, Kwangmin Kim, Keum Seok Bae, Hongjin Shim","doi":"10.4266/acc.2022.01515","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of intravenous immunoglobulin (IVIG) in sepsis patients from bowel perforation is still debatable. However, few studies have evaluated the effect of IVIG as an adjuvant therapy after source control. This study aimed to analyze the effect of IVIG in critically ill patients who underwent surgery due to secondary peritonitis.</p><p><strong>Methods: </strong>In total, 646 medical records of surgical patients who were treated for secondary peritonitis were retrospectively analyzed. IVIG use, initial clinical data, and changes in Sequential Organ Failure Assessment (SOFA) score over the 7-day admission in the intensive care unit for sepsis check, base excess, and delta neutrophil index (DNI) were analyzed. Mortalities and periodic profiles were assessed. Propensity scoring matching as comparative analysis was performed in the IVIG group and non-IVIG group.</p><p><strong>Results: </strong>General characteristics were not different between the two groups. The survival curve did not show a significantly reduced mortality in the IVIG. Moreover, the IVIG group did not have a lower risk ratio for mortality than the non-IVIG group. However, when the DNI were compared during the first 7 days, the reduction rate in the IVIG group was statistically faster than in the non-IVIG group (P<0.01).</p><p><strong>Conclusions: </strong>The use of IVIG was significantly associated with faster decrease in DNI which means faster reduction of inflammation. Since the immune system is rapidly activated, the additional use of IVIG after source control surgery in abdominal sepsis patients, especially those with immunocompromised patients can be considered. However, furthermore clinical studies are needed.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":null,"pages":null},"PeriodicalIF":1.7000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/57/17/acc-2022-01515.PMC10030247.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2022.01515","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The use of intravenous immunoglobulin (IVIG) in sepsis patients from bowel perforation is still debatable. However, few studies have evaluated the effect of IVIG as an adjuvant therapy after source control. This study aimed to analyze the effect of IVIG in critically ill patients who underwent surgery due to secondary peritonitis.
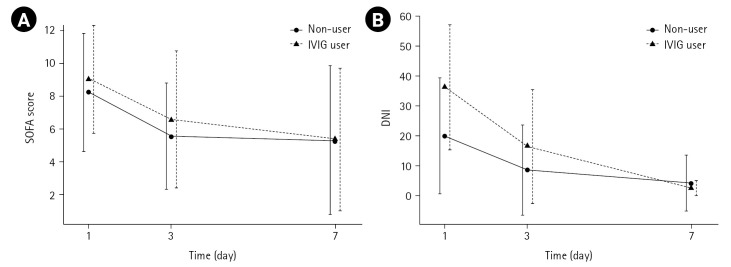
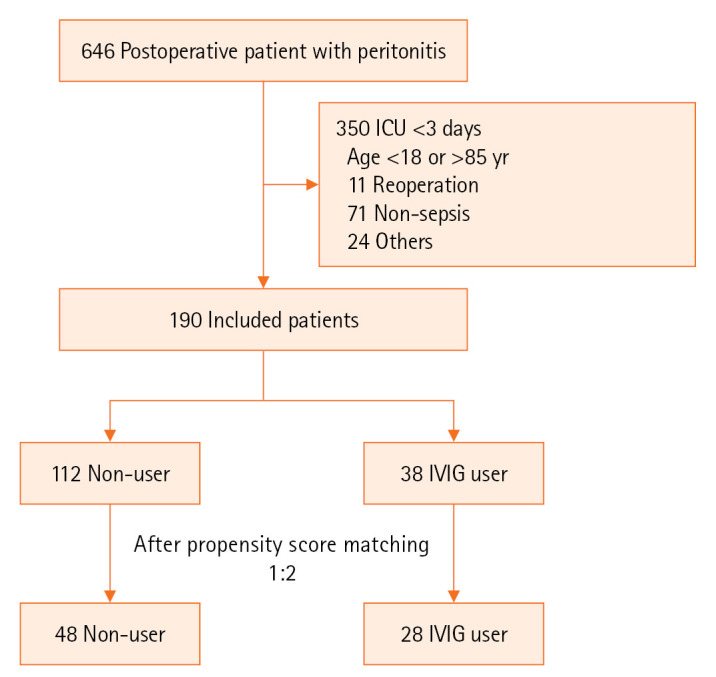
Methods: In total, 646 medical records of surgical patients who were treated for secondary peritonitis were retrospectively analyzed. IVIG use, initial clinical data, and changes in Sequential Organ Failure Assessment (SOFA) score over the 7-day admission in the intensive care unit for sepsis check, base excess, and delta neutrophil index (DNI) were analyzed. Mortalities and periodic profiles were assessed. Propensity scoring matching as comparative analysis was performed in the IVIG group and non-IVIG group.
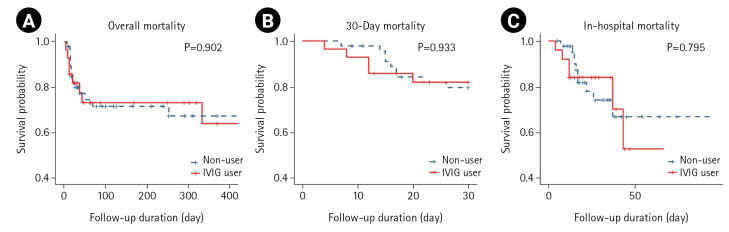
Results: General characteristics were not different between the two groups. The survival curve did not show a significantly reduced mortality in the IVIG. Moreover, the IVIG group did not have a lower risk ratio for mortality than the non-IVIG group. However, when the DNI were compared during the first 7 days, the reduction rate in the IVIG group was statistically faster than in the non-IVIG group (P<0.01).
Conclusions: The use of IVIG was significantly associated with faster decrease in DNI which means faster reduction of inflammation. Since the immune system is rapidly activated, the additional use of IVIG after source control surgery in abdominal sepsis patients, especially those with immunocompromised patients can be considered. However, furthermore clinical studies are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


