An evaluation of feeding practices and determination of barriers to providing nutritional support in a multidisciplinary South African intensive care unit.
{"title":"An evaluation of feeding practices and determination of barriers to providing nutritional support in a multidisciplinary South African intensive care unit.","authors":"E Elmezoughi, K de Vasconcellos","doi":"10.7196/SAJCC.2020.v36i1.412","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adequate nutritional support is crucial to optimising intensive care unit (ICU) outcomes.</p><p><strong>Objectives: </strong>To assess adherence to current nutritional guidelines in critically ill patients in South Africa (SA). To identify risk factors for non-adherence to guideline.</p><p><strong>Methods: </strong>Retrospective observational chart review of nutritional practices, from 1 December 2017 to 31 May 2018, during the first week of ICU admission in adult patients admitted to a tertiary, multidisciplinary ICU in Durban, SA, for >48 hours.</p><p><strong>Results: </strong>The study cohort (N=150) had a median age of 39 years and an ICU mortality of 28%. Surgical patients accounted for 50.7% of admissions. Ninety-eight percent of patients received mechanical ventilation, 75% required inotropic support, and 56% had acute kidney injury. The median time to initiation of enteral nutrition (EN) was 3 days, with EN being initiated within 48 hours in 39% of patients, and by day 7 80% of patients had received EN. Goal feeds were reached in 23% of patients by discharge, death or day 7. Parenteral nutrition was initiated in 16.7% of patients. There was an association between shock, acute kidney injury, increasing sequential organ failure assessment score and inotrope dose, and failure to initiate EN. Failure to initiate EN was predominantly due to unavoidable factors, but a number of clinical and administrative areas were identified to improve EN delivery.</p><p><strong>Conclusion: </strong>Adequate nutrition is associated with reduced morbidity, ICU length of stay, mortality and improved functional outcomes. More attention to avoiding barriers to adequate ICU nutrition and enhanced adherence to feeding protocols should be encouraged.</p><p><strong>Contributions of the study: </strong>This study significantly adds to the limited data available from sub- Saharan Africa on nutritional practices in critical care, and in particular barriers to provision of EN. It is further anticipated that the findings of the study will contribute in making recommendations in an attempt to improve the outcomes.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":"36 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.7196/SAJCC.2020.v36i1.412","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2020.v36i1.412","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adequate nutritional support is crucial to optimising intensive care unit (ICU) outcomes.
Objectives: To assess adherence to current nutritional guidelines in critically ill patients in South Africa (SA). To identify risk factors for non-adherence to guideline.
Methods: Retrospective observational chart review of nutritional practices, from 1 December 2017 to 31 May 2018, during the first week of ICU admission in adult patients admitted to a tertiary, multidisciplinary ICU in Durban, SA, for >48 hours.
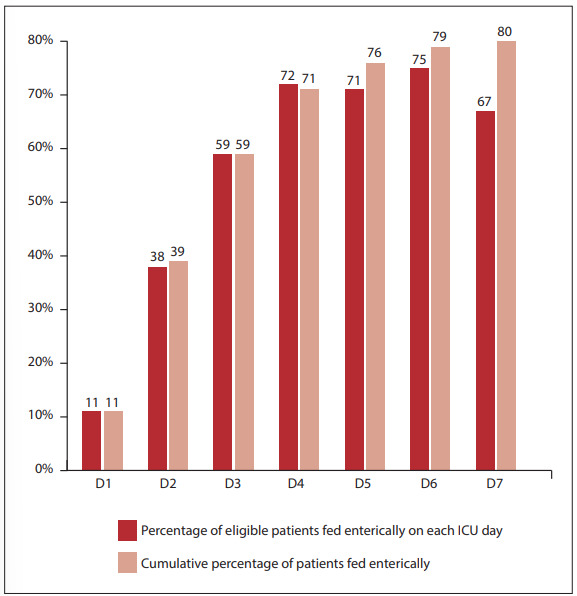
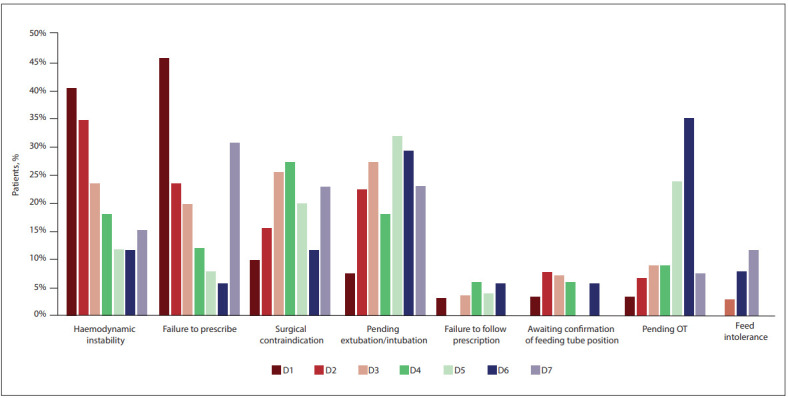
Results: The study cohort (N=150) had a median age of 39 years and an ICU mortality of 28%. Surgical patients accounted for 50.7% of admissions. Ninety-eight percent of patients received mechanical ventilation, 75% required inotropic support, and 56% had acute kidney injury. The median time to initiation of enteral nutrition (EN) was 3 days, with EN being initiated within 48 hours in 39% of patients, and by day 7 80% of patients had received EN. Goal feeds were reached in 23% of patients by discharge, death or day 7. Parenteral nutrition was initiated in 16.7% of patients. There was an association between shock, acute kidney injury, increasing sequential organ failure assessment score and inotrope dose, and failure to initiate EN. Failure to initiate EN was predominantly due to unavoidable factors, but a number of clinical and administrative areas were identified to improve EN delivery.
Conclusion: Adequate nutrition is associated with reduced morbidity, ICU length of stay, mortality and improved functional outcomes. More attention to avoiding barriers to adequate ICU nutrition and enhanced adherence to feeding protocols should be encouraged.
Contributions of the study: This study significantly adds to the limited data available from sub- Saharan Africa on nutritional practices in critical care, and in particular barriers to provision of EN. It is further anticipated that the findings of the study will contribute in making recommendations in an attempt to improve the outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


