Haris Patail, Ritika Kompella, Nicole E Hoover, Wyona Reis, Rohit Masih, Jeff F Mather, Trevor S Sutton, Raymond G McKay
{"title":"In-Hospital and One-Year Outcomes of Transcatheter Aortic Valve Replacement in Patients Requiring Supplemental Home Oxygen Use.","authors":"Haris Patail, Ritika Kompella, Nicole E Hoover, Wyona Reis, Rohit Masih, Jeff F Mather, Trevor S Sutton, Raymond G McKay","doi":"10.14740/cr1497","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There have been limited reports with inconsistent results on the impact of long-term use of oxygen therapry (LTOT) in patients treated with transcatheter aortic valve replacement (TAVR).</p><p><strong>Methods: </strong>We compared in-hospital and intermediate TAVR outcomes in 150 patients requiring LTOT (home O<sub>2</sub> cohort) with 2,313 non-home O<sub>2</sub> patients.</p><p><strong>Results: </strong>Home O<sub>2</sub> patients were younger, and had more comorbidities including chronic obstructive pulmonary disease (COPD), diabetes, carotid artery disease, lower forced expiratory volume (FEV<sub>1</sub>) (50.3±21.1% vs. 75.0±24.7%, P < 0.001), and lower diffusion capacity (DLCO, 48.6±19.2% vs. 74.6±22.4%, P < 0.001). These differences represented higher baseline Society of Thoracic Surgeons (STS) risk score (15.5±10.2% vs. 9.3±7.0%, P < 0.001) and lower pre-procedure Kansas City Cardiomyopathy Questionnaire (KCCQ-12) scores (32.5 ± 22.2 vs. 49.1 ± 25.4, P < 0.001). The home O<sub>2</sub> cohort required higher use of alternative TAVR vascular access (24.0% vs. 12.8%, P = 0.002) and general anesthesia (51.3% vs. 36.0%, P < 0.001). Compared to non-home O<sub>2</sub> patients, home O<sub>2</sub> patients showed increased in-hospital mortality (5.3% vs. 1.6%, P = 0.001), procedural cardiac arrest (4.7% vs. 1.0%, P < 0.001), and postoperative atrial fibrillation (4.0% vs. 1.5%, P = 0.013). At 1-year follow-up, the home O<sub>2</sub> cohort had a higher all-cause mortality (17.3% vs. 7.5%, P < 0.001) and lower KCCQ-12 scores (69.5 ± 23.8 vs. 82.1 ± 19.4, P < 0.001). Kaplan-Meir analysis revealed a lower survival rate in the home O<sub>2</sub> cohort with an overall mean (95% confidence interval (CI)) survival time of 6.2 (5.9 - 6.5) years (P < 0.001).</p><p><strong>Conclusion: </strong>Home O<sub>2</sub> patients represent a high-risk TAVR cohort with increased in-hospital morbidity and mortality, less improvement in 1-year KCCQ-12, and increased mortality at intermediate follow-up.</p>","PeriodicalId":9424,"journal":{"name":"Cardiology Research","volume":"14 3","pages":"228-236"},"PeriodicalIF":1.4000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3e/18/cr-14-228.PMC10257506.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/cr1497","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There have been limited reports with inconsistent results on the impact of long-term use of oxygen therapry (LTOT) in patients treated with transcatheter aortic valve replacement (TAVR).
Methods: We compared in-hospital and intermediate TAVR outcomes in 150 patients requiring LTOT (home O2 cohort) with 2,313 non-home O2 patients.
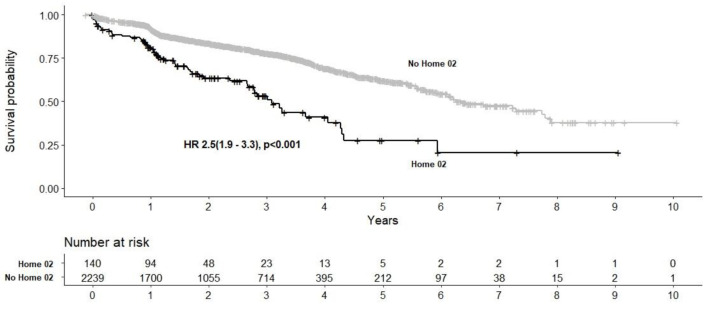
Results: Home O2 patients were younger, and had more comorbidities including chronic obstructive pulmonary disease (COPD), diabetes, carotid artery disease, lower forced expiratory volume (FEV1) (50.3±21.1% vs. 75.0±24.7%, P < 0.001), and lower diffusion capacity (DLCO, 48.6±19.2% vs. 74.6±22.4%, P < 0.001). These differences represented higher baseline Society of Thoracic Surgeons (STS) risk score (15.5±10.2% vs. 9.3±7.0%, P < 0.001) and lower pre-procedure Kansas City Cardiomyopathy Questionnaire (KCCQ-12) scores (32.5 ± 22.2 vs. 49.1 ± 25.4, P < 0.001). The home O2 cohort required higher use of alternative TAVR vascular access (24.0% vs. 12.8%, P = 0.002) and general anesthesia (51.3% vs. 36.0%, P < 0.001). Compared to non-home O2 patients, home O2 patients showed increased in-hospital mortality (5.3% vs. 1.6%, P = 0.001), procedural cardiac arrest (4.7% vs. 1.0%, P < 0.001), and postoperative atrial fibrillation (4.0% vs. 1.5%, P = 0.013). At 1-year follow-up, the home O2 cohort had a higher all-cause mortality (17.3% vs. 7.5%, P < 0.001) and lower KCCQ-12 scores (69.5 ± 23.8 vs. 82.1 ± 19.4, P < 0.001). Kaplan-Meir analysis revealed a lower survival rate in the home O2 cohort with an overall mean (95% confidence interval (CI)) survival time of 6.2 (5.9 - 6.5) years (P < 0.001).
Conclusion: Home O2 patients represent a high-risk TAVR cohort with increased in-hospital morbidity and mortality, less improvement in 1-year KCCQ-12, and increased mortality at intermediate follow-up.
期刊介绍:
Cardiology Research is an open access, peer-reviewed, international journal. All submissions relating to basic research and clinical practice of cardiology and cardiovascular medicine are in this journal''s scope. This journal focuses on publishing original research and observations in all cardiovascular medicine aspects. Manuscript types include original article, review, case report, short communication, book review, letter to the editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


