{"title":"Unexpected recovery from complete deafness to normal hearing post surgical excision of a cerebellopontine angle meningioma: A case report.","authors":"Campbell Chukwuebuka Francis, Kohei Kanaya, Hiromu Murase, Ridzky Firmansyah Hardian, Tetsuyoshi Horiuchi, Samuel Chukwunonyerem Ohaegbulam","doi":"10.25259/SNI_276_2023","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cerebellopontine angle (CPA) meningioma presents a significant management challenge due to its intricate relationship with the brainstem neurovascular bundles. The emphasis in the past has been on facial nerve preservation, but the current management standard is hearing preservation in patients with serviceable hearing; however, hearing restoration after complete loss is rare. We report an elderly man who had restoration of hearing in the right ear after complete loss following tumor resection through the retrosigmoid route.</p><p><strong>Case description: </strong>A 73-year-old male patient presented with progressive hearing impairment in the right ear, culminating in hearing loss for about 2 months (the American Academy of Otolaryngology-Head and Neck Surgery [AAO-HNS] class D). He also had mild cerebellar symptoms, but other cranial nerves and long tracts were normal. Brain magnetic resonance imaging confirmed a right CPA meningioma, and he had tumor resection through the retrosigmoid route using meticulous microsurgical technique with vestibulocochlear nerve preservation, facial nerve monitoring, and intraoperative video angiography. He had restoration of hearing on follow-up (the American Academy of Otolaryngology-Head and Neck Surgery class A). Histology confirmed World Health Organization central nervous system grade 1 meningioma.</p><p><strong>Conclusion: </strong>This case illustrates that hearing restoration is possible after complete loss in patients with CPA meningioma. We advocate hearing preservation surgery even in patients with non-serviceable hearing, as the chance of hearing recovery is possible.</p>","PeriodicalId":38981,"journal":{"name":"Surgical Neurology International","volume":"14 ","pages":"174"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1d/c3/SNI-14-174.PMC10246372.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_276_2023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cerebellopontine angle (CPA) meningioma presents a significant management challenge due to its intricate relationship with the brainstem neurovascular bundles. The emphasis in the past has been on facial nerve preservation, but the current management standard is hearing preservation in patients with serviceable hearing; however, hearing restoration after complete loss is rare. We report an elderly man who had restoration of hearing in the right ear after complete loss following tumor resection through the retrosigmoid route.
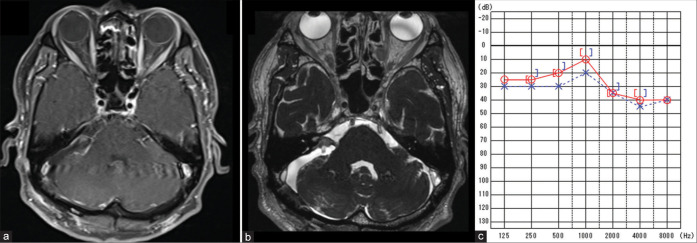
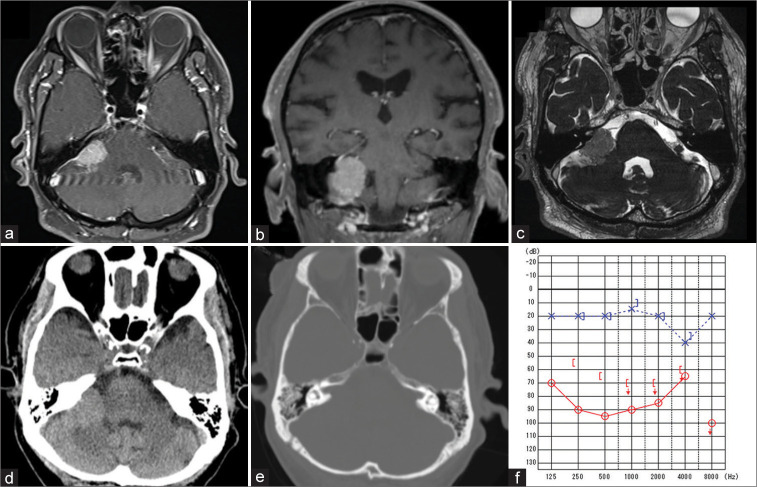
Case description: A 73-year-old male patient presented with progressive hearing impairment in the right ear, culminating in hearing loss for about 2 months (the American Academy of Otolaryngology-Head and Neck Surgery [AAO-HNS] class D). He also had mild cerebellar symptoms, but other cranial nerves and long tracts were normal. Brain magnetic resonance imaging confirmed a right CPA meningioma, and he had tumor resection through the retrosigmoid route using meticulous microsurgical technique with vestibulocochlear nerve preservation, facial nerve monitoring, and intraoperative video angiography. He had restoration of hearing on follow-up (the American Academy of Otolaryngology-Head and Neck Surgery class A). Histology confirmed World Health Organization central nervous system grade 1 meningioma.
Conclusion: This case illustrates that hearing restoration is possible after complete loss in patients with CPA meningioma. We advocate hearing preservation surgery even in patients with non-serviceable hearing, as the chance of hearing recovery is possible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


