{"title":"An Interfering Substance in Gel Tubes Affects Vitamin D Measurement by HPLC.","authors":"Mohammad Reza Haeri, Narges Emamnejad","doi":"10.4103/abr.abr_252_22","DOIUrl":null,"url":null,"abstract":"The demand for measuring vitamin D has increased dramatically, thus vitamin D measurement is one of the most frequently requested laboratory tests.[1] One of the most common methods to measure 25‐hydroxy vitamin D3 (25‐OH‐D3) is high‐performance liquid chromatography (HPLC) with enough reliability and high selectivity.[2] There is little information about the potential impact of blood collection tubes on 25(OH) D3 concentrations. However, many factors may affect the accuracy of the measurements, mainly pre‐analytical variables such as sample type and interfering factors.[3] The type of blood samples (plasma or serum) or collecting tube (plain or clot‐activating tube) sent from the hospital wards to the laboratory may vary, depending on the tests requested for the patient. The question of this study was whether the amounts of 25(OH) D3 measured by the HPLC method in serum (prepared in tubes containing gel and clot activator) and plasma are the same. For this purpose, blood samples from eight patients were collected simultaneously in tubes containing gel and clot activator, and in tubes containing EDTA (without gel). All tubes were centrifuged for 10 min at 3000 × g. Further, 25(OH) D3 was measured in all samples by HPLC (Agilent, USA) equipped with a C18 column and ultraviolet (UV) detector adjusted to 264 nm.[4] The mobile phase consisted of acetonitrile/methanol (90/10). To prepare samples, 400 μL of the patient sample and 400 μL of the precipitation and extraction reagents were dispensed into test tubes. To obtain a precipitate, the tubes were vortex‐mixed for 10 s and centrifuged at 10,000 RCF for 5 min. Finally, 250 microliters from the supernatant were injected into the HPLC, the mobile phase was applied with a flow rate of 1 mL/min in isocratic elution mode. Results were compared with the student’s t‐test using the GraphPad Prism 8.2.1 software. The significance level was defined as P ≤ 0.05.","PeriodicalId":7225,"journal":{"name":"Advanced Biomedical Research","volume":"12 ","pages":"104"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/08/d9/ABR-12-104.PMC10241623.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advanced Biomedical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/abr.abr_252_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
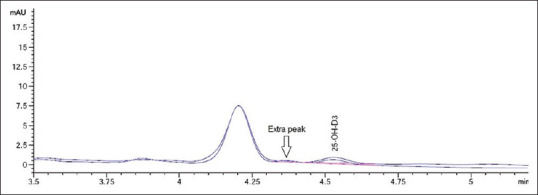
The demand for measuring vitamin D has increased dramatically, thus vitamin D measurement is one of the most frequently requested laboratory tests.[1] One of the most common methods to measure 25‐hydroxy vitamin D3 (25‐OH‐D3) is high‐performance liquid chromatography (HPLC) with enough reliability and high selectivity.[2] There is little information about the potential impact of blood collection tubes on 25(OH) D3 concentrations. However, many factors may affect the accuracy of the measurements, mainly pre‐analytical variables such as sample type and interfering factors.[3] The type of blood samples (plasma or serum) or collecting tube (plain or clot‐activating tube) sent from the hospital wards to the laboratory may vary, depending on the tests requested for the patient. The question of this study was whether the amounts of 25(OH) D3 measured by the HPLC method in serum (prepared in tubes containing gel and clot activator) and plasma are the same. For this purpose, blood samples from eight patients were collected simultaneously in tubes containing gel and clot activator, and in tubes containing EDTA (without gel). All tubes were centrifuged for 10 min at 3000 × g. Further, 25(OH) D3 was measured in all samples by HPLC (Agilent, USA) equipped with a C18 column and ultraviolet (UV) detector adjusted to 264 nm.[4] The mobile phase consisted of acetonitrile/methanol (90/10). To prepare samples, 400 μL of the patient sample and 400 μL of the precipitation and extraction reagents were dispensed into test tubes. To obtain a precipitate, the tubes were vortex‐mixed for 10 s and centrifuged at 10,000 RCF for 5 min. Finally, 250 microliters from the supernatant were injected into the HPLC, the mobile phase was applied with a flow rate of 1 mL/min in isocratic elution mode. Results were compared with the student’s t‐test using the GraphPad Prism 8.2.1 software. The significance level was defined as P ≤ 0.05.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


