Eloise Galzin , Laurent Roche , Anna Vlachomitrou , Olivier Nempont , Heike Carolus , Alexander Schmidt-Richberg , Peng Jin , Pedro Rodrigues , Tobias Klinder , Jean-Christophe Richard , Karim Tazarourte , Marion Douplat , Alain Sigal , Maude Bouscambert-Duchamp , Salim Aymeric Si-Mohamed , Sylvain Gouttard , Adeline Mansuy , François Talbot , Jean-Baptiste Pialat , Olivier Rouvière , Loic Boussel
{"title":"Additional value of chest CT AI-based quantification of lung involvement in predicting death and ICU admission for COVID-19 patients","authors":"Eloise Galzin , Laurent Roche , Anna Vlachomitrou , Olivier Nempont , Heike Carolus , Alexander Schmidt-Richberg , Peng Jin , Pedro Rodrigues , Tobias Klinder , Jean-Christophe Richard , Karim Tazarourte , Marion Douplat , Alain Sigal , Maude Bouscambert-Duchamp , Salim Aymeric Si-Mohamed , Sylvain Gouttard , Adeline Mansuy , François Talbot , Jean-Baptiste Pialat , Olivier Rouvière , Loic Boussel","doi":"10.1016/j.redii.2022.100018","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><p>We evaluated the contribution of lung lesion quantification on chest CT using a clinical Artificial Intelligence (AI) software in predicting death and intensive care units (ICU) admission for COVID-19 patients.</p></div><div><h3>Methods</h3><p>For 349 patients with positive COVID-19-PCR test that underwent a chest CT scan at admittance or during hospitalization, we applied the AI for lung and lung lesion segmentation to obtain lesion volume (LV), and LV/Total Lung Volume (TLV) ratio. ROC analysis was used to extract the best CT criterion in predicting death and ICU admission. Two prognostic models using multivariate logistic regressions were constructed to predict each outcome and were compared using AUC values. The first model (“Clinical”) was based on patients’ characteristics and clinical symptoms only. The second model (“Clinical+LV/TLV”) included also the best CT criterion.</p></div><div><h3>Results</h3><p>LV/TLV ratio demonstrated best performance for both outcomes; AUC of 67.8% (95% CI: 59.5 - 76.1) and 81.1% (95% CI: 75.7 - 86.5) respectively. Regarding death prediction, AUC values were 76.2% (95% CI: 69.9 - 82.6) and 79.9% (95%IC: 74.4 - 85.5) for the “Clinical” and the “Clinical+LV/TLV” models respectively, showing significant performance increase (+ 3.7%; p-value<0.001) when adding LV/TLV ratio. Similarly, for ICU admission prediction, AUC values were 74.9% (IC 95%: 69.2 - 80.6) and 84.8% (IC 95%: 80.4 - 89.2) respectively corresponding to significant performance increase (+ 10%: p-value<0.001).</p></div><div><h3>Conclusions</h3><p>Using a clinical AI software to quantify the COVID-19 lung involvement on chest CT, combined with clinical variables, allows better prediction of death and ICU admission.</p></div>","PeriodicalId":74676,"journal":{"name":"Research in diagnostic and interventional imaging","volume":"4 ","pages":"Article 100018"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9716289/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Research in diagnostic and interventional imaging","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2772652522000187","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives
We evaluated the contribution of lung lesion quantification on chest CT using a clinical Artificial Intelligence (AI) software in predicting death and intensive care units (ICU) admission for COVID-19 patients.
Methods
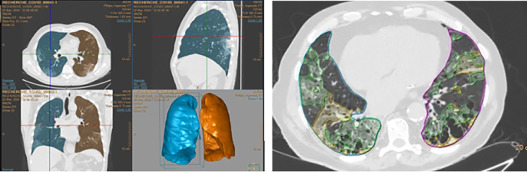
For 349 patients with positive COVID-19-PCR test that underwent a chest CT scan at admittance or during hospitalization, we applied the AI for lung and lung lesion segmentation to obtain lesion volume (LV), and LV/Total Lung Volume (TLV) ratio. ROC analysis was used to extract the best CT criterion in predicting death and ICU admission. Two prognostic models using multivariate logistic regressions were constructed to predict each outcome and were compared using AUC values. The first model (“Clinical”) was based on patients’ characteristics and clinical symptoms only. The second model (“Clinical+LV/TLV”) included also the best CT criterion.
Results
LV/TLV ratio demonstrated best performance for both outcomes; AUC of 67.8% (95% CI: 59.5 - 76.1) and 81.1% (95% CI: 75.7 - 86.5) respectively. Regarding death prediction, AUC values were 76.2% (95% CI: 69.9 - 82.6) and 79.9% (95%IC: 74.4 - 85.5) for the “Clinical” and the “Clinical+LV/TLV” models respectively, showing significant performance increase (+ 3.7%; p-value<0.001) when adding LV/TLV ratio. Similarly, for ICU admission prediction, AUC values were 74.9% (IC 95%: 69.2 - 80.6) and 84.8% (IC 95%: 80.4 - 89.2) respectively corresponding to significant performance increase (+ 10%: p-value<0.001).
Conclusions
Using a clinical AI software to quantify the COVID-19 lung involvement on chest CT, combined with clinical variables, allows better prediction of death and ICU admission.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


