A near-miss diagnosis of necrotizing breast fasciitis complicated by atrial fibrillation secondary to septic focus: a case report and brief review of literature.
IF 0.5 Q4 RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
Rachel Jane Klapper, Benjamin Joseph Michael Horn, Benedict Amalraj, Maamannan Venkataraj, Mohammad Abdurrehman Sheikh, Dominika Pullmann, Kiran Malikayil, Jeffrey Wooliscroft
{"title":"A near-miss diagnosis of necrotizing breast fasciitis complicated by atrial fibrillation secondary to septic focus: a case report and brief review of literature.","authors":"Rachel Jane Klapper, Benjamin Joseph Michael Horn, Benedict Amalraj, Maamannan Venkataraj, Mohammad Abdurrehman Sheikh, Dominika Pullmann, Kiran Malikayil, Jeffrey Wooliscroft","doi":"10.1259/bjrcr.20220120","DOIUrl":null,"url":null,"abstract":"<p><p>Necrotizing fasciitis of the breast is a rare, life-threatening entity characterized by a rapidly aggressive infection of the soft tissue. There are few literature reports on necrotizing fasciitis at the level of the breast tissue as the most common locations are within the abdominal wall or extremities, but this entity can lead to sepsis and systemic multiorgan failure if not adequately managed. Here, we report a case that highlights the course of a 68-year-old African American female with a past medical history of hypertension, hyperlipidemia, and poorly controlled diabetes mellitus, who presented with the complaint of a painful right breast abscess with intermittent, purulent drainage. An initial point-of-care ultrasound displayed an area of induration of the right breast as well as soft tissue edema with no identifiable fluid collection. A subsequent CT abdomen and pelvis was obtained given new onset abdominal pain, which demonstrated incidental findings of inflammatory changes and subcutaneous emphysema along with colonic diverticulosis. Surgical intervention was immediately sought for which she underwent debridement and exploration of the right breast with findings that were consistent with necrotizing transformation. The patient was sent back to the OR for an additional surgical debridement the next day. Of note, the patient had post-op atrial fibrillation with rapid ventricular response and had to be admitted to the ICU for conversion to sinus rhythm. She returned to sinus rhythm and was transferred back to medicine before application of a negative pressure wound dressing on discharge. The patient was transitioned from Enoxaparin to Apixaban for anticoagulation control in the setting of atrial fibrillation before being discharged to a Skilled Nursing Facility with long-term antibiotics. This case highlights the difficulty and significance in establishing a prompt diagnosis for necrotizing fasciitis.</p>","PeriodicalId":45216,"journal":{"name":"BJR Case Reports","volume":"9 2","pages":"20220120"},"PeriodicalIF":0.5000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10043598/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1259/bjrcr.20220120","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
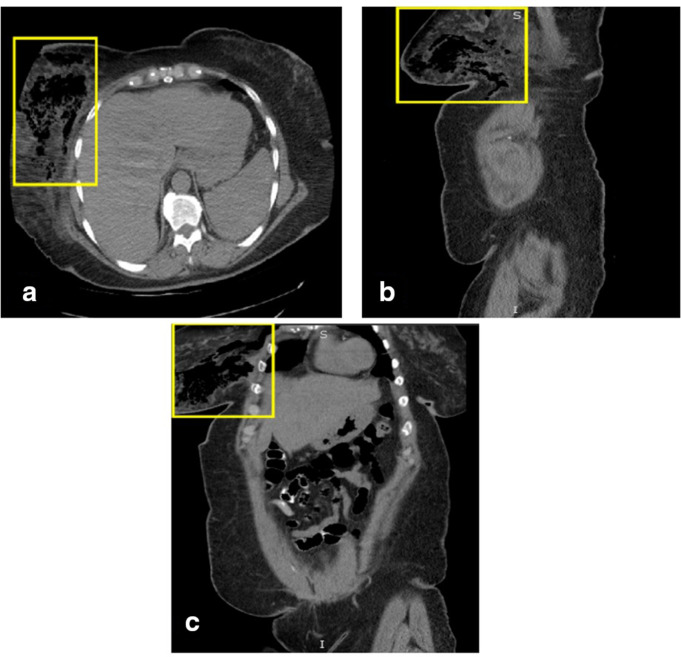
Necrotizing fasciitis of the breast is a rare, life-threatening entity characterized by a rapidly aggressive infection of the soft tissue. There are few literature reports on necrotizing fasciitis at the level of the breast tissue as the most common locations are within the abdominal wall or extremities, but this entity can lead to sepsis and systemic multiorgan failure if not adequately managed. Here, we report a case that highlights the course of a 68-year-old African American female with a past medical history of hypertension, hyperlipidemia, and poorly controlled diabetes mellitus, who presented with the complaint of a painful right breast abscess with intermittent, purulent drainage. An initial point-of-care ultrasound displayed an area of induration of the right breast as well as soft tissue edema with no identifiable fluid collection. A subsequent CT abdomen and pelvis was obtained given new onset abdominal pain, which demonstrated incidental findings of inflammatory changes and subcutaneous emphysema along with colonic diverticulosis. Surgical intervention was immediately sought for which she underwent debridement and exploration of the right breast with findings that were consistent with necrotizing transformation. The patient was sent back to the OR for an additional surgical debridement the next day. Of note, the patient had post-op atrial fibrillation with rapid ventricular response and had to be admitted to the ICU for conversion to sinus rhythm. She returned to sinus rhythm and was transferred back to medicine before application of a negative pressure wound dressing on discharge. The patient was transitioned from Enoxaparin to Apixaban for anticoagulation control in the setting of atrial fibrillation before being discharged to a Skilled Nursing Facility with long-term antibiotics. This case highlights the difficulty and significance in establishing a prompt diagnosis for necrotizing fasciitis.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


