Andrew D. Hawkins MD , Raymond J. Strobel MD, MSc , J. Hunter Mehaffey MD, MSc , Robert B. Hawkins MD, MSc , Evan P. Rotar MD, MS , Andrew M. Young MD , Leora T. Yarboro MD , Kenan Yount MD, MBA , Gorav Ailawadi MD, MBA , Mark Joseph MD , Mohammed Quader MD , Nicholas R. Teman MD
{"title":"Operating Room Versus Intensive Care Unit Extubation Within 6 Hours After On-Pump Cardiac Surgery: Early Results and Hospital Costs","authors":"Andrew D. Hawkins MD , Raymond J. Strobel MD, MSc , J. Hunter Mehaffey MD, MSc , Robert B. Hawkins MD, MSc , Evan P. Rotar MD, MS , Andrew M. Young MD , Leora T. Yarboro MD , Kenan Yount MD, MBA , Gorav Ailawadi MD, MBA , Mark Joseph MD , Mohammed Quader MD , Nicholas R. Teman MD","doi":"10.1053/j.semtcvs.2022.09.013","DOIUrl":null,"url":null,"abstract":"<div><p><span>Time-directed extubation<span> (fast-track) protocols may decrease length of stay and cost but data on operating room (OR) extubation is limited. The objective of this study was to compare the outcomes of extubation in the OR versus fast-track extubation within 6 hours of leaving the operating room. Patients undergoing nonemergent STS index cases (2011–2021) who were extubated within 6 hours were identified from a regional STS quality collaborative. Patients were stratified by extubation in the OR versus fast track. Propensity score matching (1:n) was performed to balance baseline differences. Of the 24,962 patients, 498 were extubated in the OR. After matching, 487 OR extubation cases and 899 fast track cases were well balanced. The rate of reintubation was higher for patients extubated in the OR [21/487 (4.3%) vs 16/899 (1.8%), </span></span><em>P</em><span> = 0.008] as was the incidence of reoperation for bleeding [12/487 (2.5%) vs 8/899 (0.9%), </span><em>P</em> = 0.03]. There was no significant difference in the rate of any reoperation [16/487 (3.3%) vs 15/899 (1.6%), <em>P</em><span> = 0.06] or operative mortality [4/487 (0.8%) vs 6/899 (0.6%), </span><em>P</em> = 0.7]. OR extubation was associated with shorter hospital length of stay (5.6 vs 6.2 days, <em>P</em> < 0.001) and lower total cost of admission ($29,602 vs $31,565 <em>P</em> < 0.001). OR extubation is associated with a higher postoperative risk of reintubation and reoperation due to bleeding, but lower resource utilization.Future research exploring predictors of extubation readiness may be required prior to widespread adoption of this practice.</p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 2","pages":"Pages 195-208"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067922002726","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
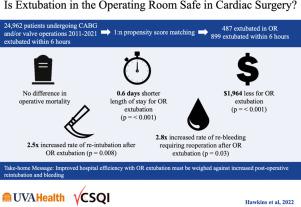
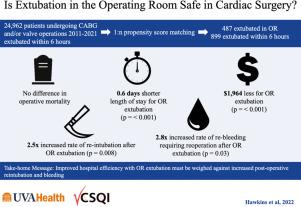
Time-directed extubation (fast-track) protocols may decrease length of stay and cost but data on operating room (OR) extubation is limited. The objective of this study was to compare the outcomes of extubation in the OR versus fast-track extubation within 6 hours of leaving the operating room. Patients undergoing nonemergent STS index cases (2011–2021) who were extubated within 6 hours were identified from a regional STS quality collaborative. Patients were stratified by extubation in the OR versus fast track. Propensity score matching (1:n) was performed to balance baseline differences. Of the 24,962 patients, 498 were extubated in the OR. After matching, 487 OR extubation cases and 899 fast track cases were well balanced. The rate of reintubation was higher for patients extubated in the OR [21/487 (4.3%) vs 16/899 (1.8%), P = 0.008] as was the incidence of reoperation for bleeding [12/487 (2.5%) vs 8/899 (0.9%), P = 0.03]. There was no significant difference in the rate of any reoperation [16/487 (3.3%) vs 15/899 (1.6%), P = 0.06] or operative mortality [4/487 (0.8%) vs 6/899 (0.6%), P = 0.7]. OR extubation was associated with shorter hospital length of stay (5.6 vs 6.2 days, P < 0.001) and lower total cost of admission ($29,602 vs $31,565 P < 0.001). OR extubation is associated with a higher postoperative risk of reintubation and reoperation due to bleeding, but lower resource utilization.Future research exploring predictors of extubation readiness may be required prior to widespread adoption of this practice.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


