Laura R Saslow, Amanda L Missel, Alison O'Brien, Sarah Kim, Frederick M Hecht, Judith T Moskowitz, Hovig Bayandorian, Martha Pietrucha, Kate Raymond, Blair Richards, Bradley Liestenfeltz, Ashley E Mason, Jennifer Daubenmier, James E Aikens
{"title":"Psychological Support Strategies for Adults With Type 2 Diabetes in a Very Low-Carbohydrate Web-Based Program: Randomized Controlled Trial.","authors":"Laura R Saslow, Amanda L Missel, Alison O'Brien, Sarah Kim, Frederick M Hecht, Judith T Moskowitz, Hovig Bayandorian, Martha Pietrucha, Kate Raymond, Blair Richards, Bradley Liestenfeltz, Ashley E Mason, Jennifer Daubenmier, James E Aikens","doi":"10.2196/44295","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A very low-carbohydrate (VLC) nutritional strategy may improve glycemic control and weight loss in adults with type 2 diabetes (T2D). However, the supplementary behavioral strategies that might be able to improve outcomes using this nutritional strategy are uncertain.</p><p><strong>Objective: </strong>This study aims to compare the impact of adding 3 different supplementary behavioral strategies to a web-based VLC diet intervention. To our knowledge, this is the first trial to randomize participants to different frequencies of dietary self-monitoring.</p><p><strong>Methods: </strong>The study included 112 overweight adults with T2D (hemoglobin A<sub>1c</sub> ≥6.5%) taking no antiglycemic medications or only metformin. They received a remotely delivered 12-month VLC diet intervention. Participants were randomly assigned through a full factorial 2×2×2 design to supplementary strategies: either daily or monthly dietary self-monitoring, either mindful eating training or not, and either positive affect skills training or not. Our research goal was to determine whether 3 different supplemental strategies had at least a medium effect size (Cohen d=0.5).</p><p><strong>Results: </strong>Overall, the VLC intervention led to statistically significant improvements in glycemic control (-0.70%, 95% CI -1.04% to -0.35%; P<.001), weight loss (-6.82%, 95% CI -8.57% to -5.08%; P<.001), and depressive symptom severity (Cohen d -0.67, 95% CI -0.92 to -0.41; P<.001). Furthermore, 30% (25/83) of the participants taking metformin at baseline reduced or discontinued their metformin. Only 1 Cohen d point estimate reached 0.5; daily (vs monthly) dietary self-monitoring had a worse impact on depressive symptoms severity (Cohen d=0.47, 95% CI -0.02 to 0.95; P=.06). None of the strategies had a statistically significant effect on outcomes. For changes in our primary outcome, hemoglobin A<sub>1c</sub>, the daily (vs monthly) dietary self-monitoring impact was 0.42% (95% CI -0.28% to 1.12%); for mindful eating, it was -0.47% (95% CI -1.15% to 0.22%); and for positive affect, it was 0.12% (95% CI -0.57% to 0.82%). Other results for daily (vs monthly) dietary self-monitoring were mixed, suggesting an increase in weight (0.98%) and depressive symptoms (Cohen d=0.47), less intervention satisfaction (Cohen d=-0.20), more sessions viewed (3.02), and greater dietary adherence (Cohen d=0.24). For mindful eating, the results suggested a benefit for dietary adherence (Cohen d=0.24) and intervention satisfaction (Cohen d=0.30). For positive affect, the results suggested a benefit for depressive symptoms (Cohen d=-0.32), the number of sessions viewed (3.68), dietary adherence (Cohen d=0.16), and intervention satisfaction (Cohen d=0.25).</p><p><strong>Conclusions: </strong>Overall, our results support the use of a VLC diet intervention in adults with T2D. The addition of monthly (not daily) dietary self-monitoring, mindful eating, and positive affect skills training did not show a definitive benefit, but it is worth further testing.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT03037528; https://clinicaltrials.gov/ct2/show/NCT03037528.</p>","PeriodicalId":52371,"journal":{"name":"JMIR Diabetes","volume":"8 ","pages":"e44295"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10214122/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Diabetes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/44295","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A very low-carbohydrate (VLC) nutritional strategy may improve glycemic control and weight loss in adults with type 2 diabetes (T2D). However, the supplementary behavioral strategies that might be able to improve outcomes using this nutritional strategy are uncertain.
Objective: This study aims to compare the impact of adding 3 different supplementary behavioral strategies to a web-based VLC diet intervention. To our knowledge, this is the first trial to randomize participants to different frequencies of dietary self-monitoring.
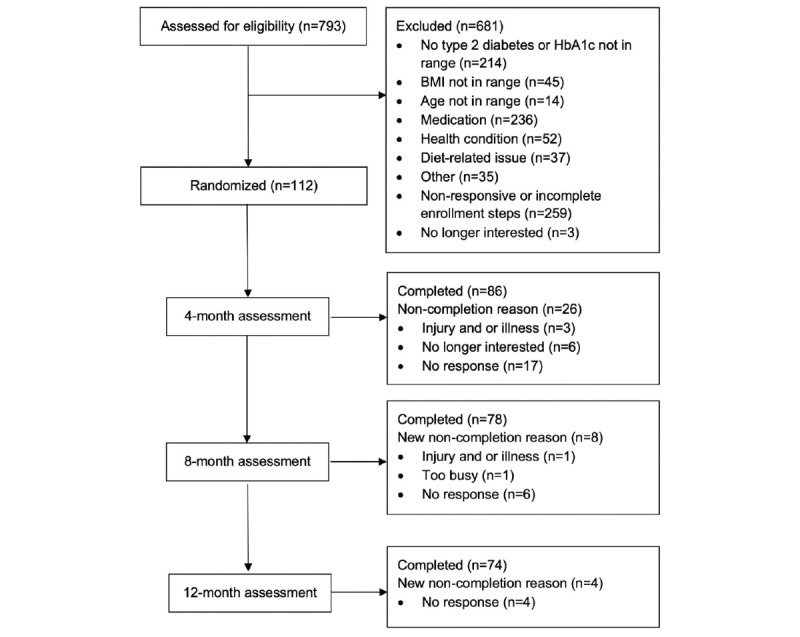
Methods: The study included 112 overweight adults with T2D (hemoglobin A1c ≥6.5%) taking no antiglycemic medications or only metformin. They received a remotely delivered 12-month VLC diet intervention. Participants were randomly assigned through a full factorial 2×2×2 design to supplementary strategies: either daily or monthly dietary self-monitoring, either mindful eating training or not, and either positive affect skills training or not. Our research goal was to determine whether 3 different supplemental strategies had at least a medium effect size (Cohen d=0.5).
Results: Overall, the VLC intervention led to statistically significant improvements in glycemic control (-0.70%, 95% CI -1.04% to -0.35%; P<.001), weight loss (-6.82%, 95% CI -8.57% to -5.08%; P<.001), and depressive symptom severity (Cohen d -0.67, 95% CI -0.92 to -0.41; P<.001). Furthermore, 30% (25/83) of the participants taking metformin at baseline reduced or discontinued their metformin. Only 1 Cohen d point estimate reached 0.5; daily (vs monthly) dietary self-monitoring had a worse impact on depressive symptoms severity (Cohen d=0.47, 95% CI -0.02 to 0.95; P=.06). None of the strategies had a statistically significant effect on outcomes. For changes in our primary outcome, hemoglobin A1c, the daily (vs monthly) dietary self-monitoring impact was 0.42% (95% CI -0.28% to 1.12%); for mindful eating, it was -0.47% (95% CI -1.15% to 0.22%); and for positive affect, it was 0.12% (95% CI -0.57% to 0.82%). Other results for daily (vs monthly) dietary self-monitoring were mixed, suggesting an increase in weight (0.98%) and depressive symptoms (Cohen d=0.47), less intervention satisfaction (Cohen d=-0.20), more sessions viewed (3.02), and greater dietary adherence (Cohen d=0.24). For mindful eating, the results suggested a benefit for dietary adherence (Cohen d=0.24) and intervention satisfaction (Cohen d=0.30). For positive affect, the results suggested a benefit for depressive symptoms (Cohen d=-0.32), the number of sessions viewed (3.68), dietary adherence (Cohen d=0.16), and intervention satisfaction (Cohen d=0.25).
Conclusions: Overall, our results support the use of a VLC diet intervention in adults with T2D. The addition of monthly (not daily) dietary self-monitoring, mindful eating, and positive affect skills training did not show a definitive benefit, but it is worth further testing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


