Ana Tejedor, Carme Deiros, Lana Bijelic, Marta García
{"title":"Wound infiltration or transversus abdominis plane block after laparoscopic radical prostatectomy: a randomized clinical trial.","authors":"Ana Tejedor, Carme Deiros, Lana Bijelic, Marta García","doi":"10.17085/apm.23005","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Regional anesthesia techniques are commonly used for postoperative pain management during laparoscopic surgery. Our aim was to compare the analgesic efficacy of pre-incisional subcutaneous wound infiltration (WI) with that of the transversus abdominis plane (TAP) block as part of a multimodal analgesic approach in laparoscopic radical prostatectomy.</p><p><strong>Methods: </strong>In this prospective, double-blinded, randomized controlled clinical trial, 60 patients were assigned to either TAP or WI group. The main outcome was acute postoperative pain control assessed using the mean numeric rating scale (NRS) at the 24 hours postoperatively. The secondary outcomes were opioid requirements, procedure-related complications, overall complications, and length of stay.</p><p><strong>Results: </strong>In this study, 60 patients were randomized: 30 to TAP group and 28 to WI (two were excluded due to conversion to open surgery). We found no significant difference in the median (1Q, 3Q) NRS scores during the 24 h postoperatively neither at rest (TAP, 0 (0, 1) vs. WI, 0 (0, 1), P = 0.812), nor during movement (TAP, 1 (0, 2) vs. WI, 1 (0, 2), P = 0.708). There were no statistical differences in the postoperative intravenous morphine requirements in the TAP vs. WI groups during the same period (1.7 ± 3.1 vs. 1.8 ± 4.1 mg; P = 0.910). Only one patient in the TAP group presented with postoperative nausea and vomiting.</p><p><strong>Conclusions: </strong>Both pre-incisional subcutaneous WI and TAP blockade were associated with very low pain scores as part of a non-opioid multimodal analgesic regimen in laparoscopic radical prostatectomy. This study did not demonstrate the benefits of WI over TAP.</p>","PeriodicalId":7801,"journal":{"name":"Anesthesia and pain medicine","volume":"18 2","pages":"190-197"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/49/24/apm-23005.PMC10183622.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.23005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Regional anesthesia techniques are commonly used for postoperative pain management during laparoscopic surgery. Our aim was to compare the analgesic efficacy of pre-incisional subcutaneous wound infiltration (WI) with that of the transversus abdominis plane (TAP) block as part of a multimodal analgesic approach in laparoscopic radical prostatectomy.
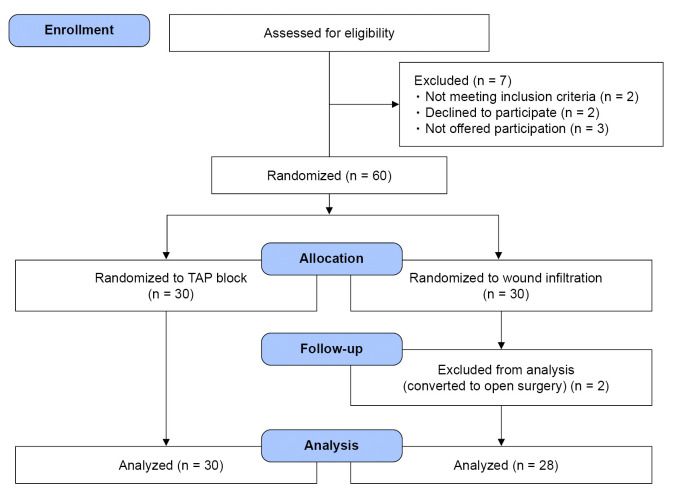
Methods: In this prospective, double-blinded, randomized controlled clinical trial, 60 patients were assigned to either TAP or WI group. The main outcome was acute postoperative pain control assessed using the mean numeric rating scale (NRS) at the 24 hours postoperatively. The secondary outcomes were opioid requirements, procedure-related complications, overall complications, and length of stay.
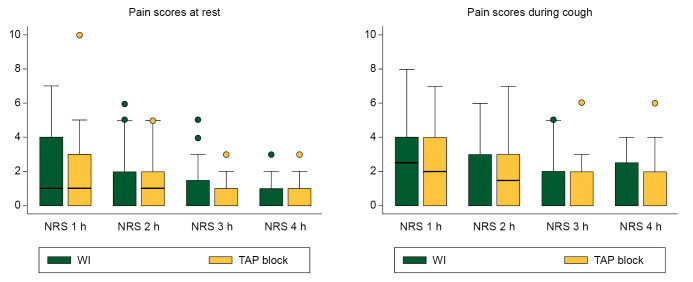
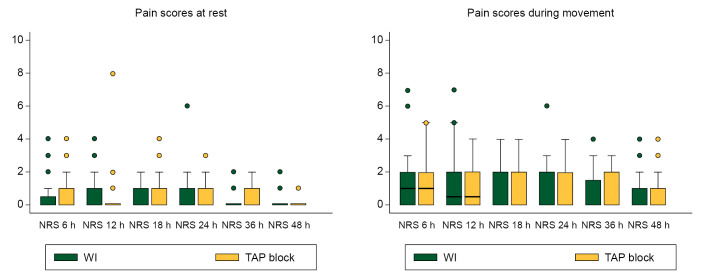
Results: In this study, 60 patients were randomized: 30 to TAP group and 28 to WI (two were excluded due to conversion to open surgery). We found no significant difference in the median (1Q, 3Q) NRS scores during the 24 h postoperatively neither at rest (TAP, 0 (0, 1) vs. WI, 0 (0, 1), P = 0.812), nor during movement (TAP, 1 (0, 2) vs. WI, 1 (0, 2), P = 0.708). There were no statistical differences in the postoperative intravenous morphine requirements in the TAP vs. WI groups during the same period (1.7 ± 3.1 vs. 1.8 ± 4.1 mg; P = 0.910). Only one patient in the TAP group presented with postoperative nausea and vomiting.
Conclusions: Both pre-incisional subcutaneous WI and TAP blockade were associated with very low pain scores as part of a non-opioid multimodal analgesic regimen in laparoscopic radical prostatectomy. This study did not demonstrate the benefits of WI over TAP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


