Ahmet Çağrı Aykan, Tayyar Gökdeniz, İlker Gül, Ezgi Kalaycıoğlu, Can Yücel Karabay, Faruk Boyacı, Engin Hatem, Scott D Weingart, İhsan Dursun
{"title":"Reduced-Dose Systemic Fibrinolysis in Massive Pulmonary Embolism: A Pilot Study.","authors":"Ahmet Çağrı Aykan, Tayyar Gökdeniz, İlker Gül, Ezgi Kalaycıoğlu, Can Yücel Karabay, Faruk Boyacı, Engin Hatem, Scott D Weingart, İhsan Dursun","doi":"10.15441/ceem.23.015","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Severe pulmonary embolism (PE) has a high mortality rate, which can be lowered by thrombolytic therapy (TT). However, full-dose TT is associated with major complications, including life-threatening bleeding. The aim of this study was to explore the efficacy and safety of extended, low-dose administration of tissue plasminogen activator (tPA) on in-hospital mortality and outcomes in massive PE.</p><p><strong>Methods: </strong>This was a single-center, prospective cohort trial at a tertiary university hospital. A total of 37 consecutive patients with massive PE were included. A peripheral intravenous infusion was used to administer 25 mg of tPA over 6 hours. The primary endpoints were in-hospital mortality, major complications, pulmonary hypertension, and right ventricular dysfunction. The secondary endpoints were 6-month mortality and pulmonary hypertension and right ventricular dysfunction 6 months after the PE.</p><p><strong>Results: </strong>The mean age of the patients was 68.76±14.54 years. The mean pulmonary artery systolic pressure (PASP; 56.51±7.34 mmHg vs. 34.16±2.81 mmHg, P<0.001) and right/left ventricle diameter (1.37±0.12 vs. 0.99±0.12, P<0.001) decreased significantly after TT. Tricuspid annular plane systolic excursion (1.43±0.33 cm vs. 2.07±0.27 cm, P<0.001), myocardial performance index (0.47±0.08 vs. 0.55±0.07, P<0.001), and systolic wave prime (9.6±2.8 vs. 15.3±2.6) increased significantly after TT. No major bleeding or stroke was observed. There was one in-hospital death and two additional deaths within 6 months. No cases of pulmonary hypertension were identified during follow-up.</p><p><strong>Conclusion: </strong>The results of this pilot study suggest that an extended infusion of low-dose tPA is a safe and effective therapy in patients with massive PE. This protocol was also effective in decreasing PASP and restoring right ventricular function.</p>","PeriodicalId":10325,"journal":{"name":"Clinical and Experimental Emergency Medicine","volume":null,"pages":null},"PeriodicalIF":1.9000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/38/28/ceem-23-015.PMC10579734.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15441/ceem.23.015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 1
Abstract
Objective: Severe pulmonary embolism (PE) has a high mortality rate, which can be lowered by thrombolytic therapy (TT). However, full-dose TT is associated with major complications, including life-threatening bleeding. The aim of this study was to explore the efficacy and safety of extended, low-dose administration of tissue plasminogen activator (tPA) on in-hospital mortality and outcomes in massive PE.
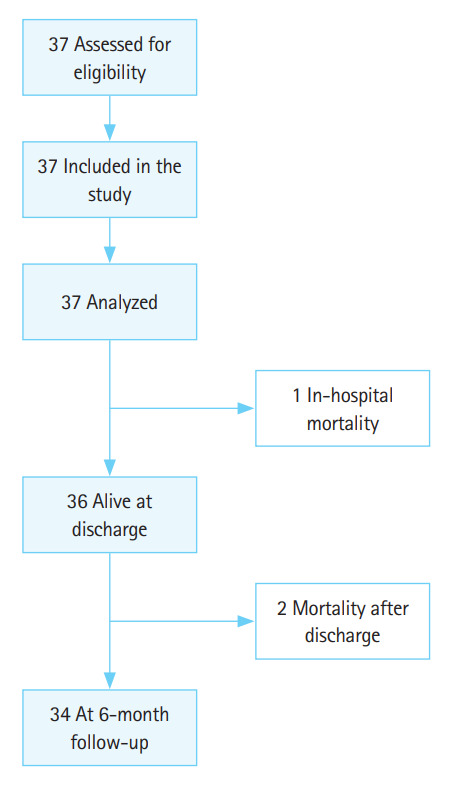
Methods: This was a single-center, prospective cohort trial at a tertiary university hospital. A total of 37 consecutive patients with massive PE were included. A peripheral intravenous infusion was used to administer 25 mg of tPA over 6 hours. The primary endpoints were in-hospital mortality, major complications, pulmonary hypertension, and right ventricular dysfunction. The secondary endpoints were 6-month mortality and pulmonary hypertension and right ventricular dysfunction 6 months after the PE.
Results: The mean age of the patients was 68.76±14.54 years. The mean pulmonary artery systolic pressure (PASP; 56.51±7.34 mmHg vs. 34.16±2.81 mmHg, P<0.001) and right/left ventricle diameter (1.37±0.12 vs. 0.99±0.12, P<0.001) decreased significantly after TT. Tricuspid annular plane systolic excursion (1.43±0.33 cm vs. 2.07±0.27 cm, P<0.001), myocardial performance index (0.47±0.08 vs. 0.55±0.07, P<0.001), and systolic wave prime (9.6±2.8 vs. 15.3±2.6) increased significantly after TT. No major bleeding or stroke was observed. There was one in-hospital death and two additional deaths within 6 months. No cases of pulmonary hypertension were identified during follow-up.
Conclusion: The results of this pilot study suggest that an extended infusion of low-dose tPA is a safe and effective therapy in patients with massive PE. This protocol was also effective in decreasing PASP and restoring right ventricular function.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


