{"title":"The Association Between Time From Emergency Department Visit to ICU Admission and Mortality in Patients With Sepsis.","authors":"Junichiro Shibata, Itsuki Osawa, Kiyoyasu Fukuchi, Tadahiro Goto","doi":"10.1097/CCE.0000000000000915","DOIUrl":null,"url":null,"abstract":"<p><p>The Surviving Sepsis Campaign Guidelines 2021 recommends that adult patients with sepsis requiring intensive care should be admitted to the ICU within 6 hours of their emergency department (ED) visits. However, there is limited evidence on whether 6 hours is the best target time for compliance with the sepsis bundle. We aimed to investigate the association between time from ED visits to ICU admission (i.e., ED length of stay [ED-LOS]) and mortality and identify the optimal ED-LOS for patients with sepsis.</p><p><strong>Design: </strong>Retrospective cohort study.</p><p><strong>Setting: </strong>The Medical Information Mart for Intensive Care Emergency Department and Medical Information Mart for Intensive Care IV databases.</p><p><strong>Patients: </strong>Adult patients (≥ 18 yr old) who were transferred from the ED to the ICU and subsequently diagnosed with sepsis based on the Sepsis-3 criteria within 24 hours of ICU admission.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>Among 1,849 patients with sepsis, we found a disproportionally higher mortality rate in patients immediately admitted to the ICU (e.g., < 2 hr). When using ED-LOS as a continuous variable, ED-LOS was not significantly associated with 28-day mortality (adjusted odds ratio [OR] per hour increase, 1.04; 95% CI, 0.96-1.13; <i>p</i> = 0.3) after an adjustment for potential confounders (e.g., demographics, triage vital signs, and laboratory results) in the multivariable analysis. However, when we categorized all patients into time quartiles (ED-LOS: < 3.3 hr, 3.3-4.5 hr, 4.6-6.1 hr, and > 6.1 hr), patients in the higher time quartiles (e.g., 3.3-4.5 hr) had higher 28-day mortality compared with those in the lowest time quartile (< 3.3 hr) (e.g., adjusted OR for patients in the second time quartile [3.3-4.5 hr] 1.59; 95% CI, 1.03-2.46; <i>p</i> = 0.04).</p><p><strong>Conclusions: </strong>Earlier admission to the ICU (e.g., within 3.3 hr of ED visits) was associated with lower 28-day mortality in patients with sepsis. Our findings suggest patients with sepsis who require intensive care may benefit from a more immediate ICU admission than 6 hours.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 5","pages":"e0915"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/35/8c/cc9-5-e0915.PMC10171575.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000915","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
The Surviving Sepsis Campaign Guidelines 2021 recommends that adult patients with sepsis requiring intensive care should be admitted to the ICU within 6 hours of their emergency department (ED) visits. However, there is limited evidence on whether 6 hours is the best target time for compliance with the sepsis bundle. We aimed to investigate the association between time from ED visits to ICU admission (i.e., ED length of stay [ED-LOS]) and mortality and identify the optimal ED-LOS for patients with sepsis.
Design: Retrospective cohort study.
Setting: The Medical Information Mart for Intensive Care Emergency Department and Medical Information Mart for Intensive Care IV databases.
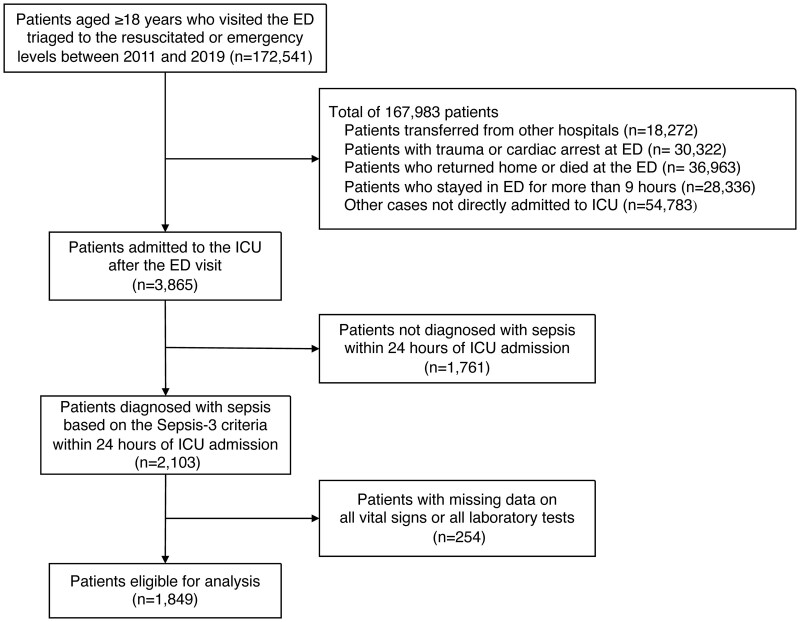
Patients: Adult patients (≥ 18 yr old) who were transferred from the ED to the ICU and subsequently diagnosed with sepsis based on the Sepsis-3 criteria within 24 hours of ICU admission.
Interventions: None.
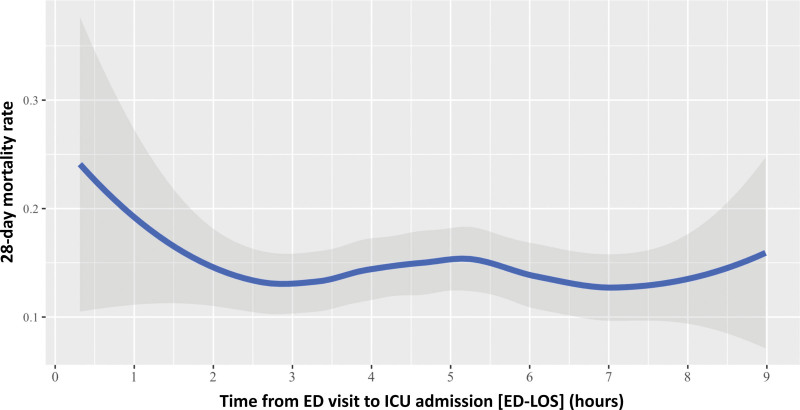
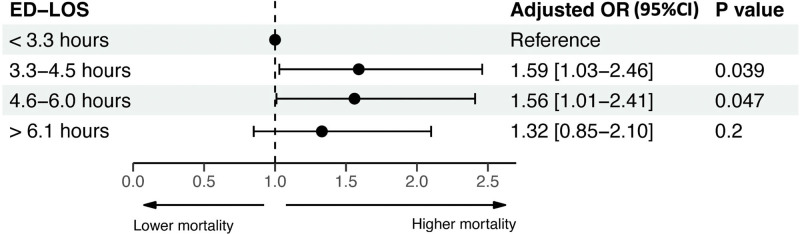
Measurements and main results: Among 1,849 patients with sepsis, we found a disproportionally higher mortality rate in patients immediately admitted to the ICU (e.g., < 2 hr). When using ED-LOS as a continuous variable, ED-LOS was not significantly associated with 28-day mortality (adjusted odds ratio [OR] per hour increase, 1.04; 95% CI, 0.96-1.13; p = 0.3) after an adjustment for potential confounders (e.g., demographics, triage vital signs, and laboratory results) in the multivariable analysis. However, when we categorized all patients into time quartiles (ED-LOS: < 3.3 hr, 3.3-4.5 hr, 4.6-6.1 hr, and > 6.1 hr), patients in the higher time quartiles (e.g., 3.3-4.5 hr) had higher 28-day mortality compared with those in the lowest time quartile (< 3.3 hr) (e.g., adjusted OR for patients in the second time quartile [3.3-4.5 hr] 1.59; 95% CI, 1.03-2.46; p = 0.04).
Conclusions: Earlier admission to the ICU (e.g., within 3.3 hr of ED visits) was associated with lower 28-day mortality in patients with sepsis. Our findings suggest patients with sepsis who require intensive care may benefit from a more immediate ICU admission than 6 hours.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


