{"title":"Thyrotropin Receptor Autoantibody Assessment in Thyroid Eye Disease: Does the Assay Type Matter?","authors":"Malik Moledina, Jonathan Roos, Rachna Murthy","doi":"10.3341/kjo.2022.0131","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Thyroid receptor antibodies can quantify thyroid eye disease activity, predict outcomes and aid timing of interventions. The type and generation of assay is frequently unspecified, complicating meta-analyses. To determine the clinical and biochemical relationships between a second-generation thyrotropin receptor-binding inhibition antibody (TRAb) immunoassay, detecting stimulatory and blocking antibodies, with the thyroid stimulating immunoglobulin (TSI) bridging immunoassay detecting the stimulatory component only.</p><p><strong>Methods: </strong>Retrospective review of 100 consecutive patients attending a regional specialist service. For each patient and visit, both a TRAb and TSI were performed, and a clinical activity score (CAS) recorded.</p><p><strong>Results: </strong>A significant positive correlation between TRAb and TSI (rho = 0.828, p < 0.01) but a weaker correlation between the assays and CAS (TRAb: rho = 0.439, p < 0.01; TSI: r = 0.357, p < 0.01) were found. In 10% of the episodic data, patients had a TRAb level that was disproportionately high (39.41 ± 52.84 IU/L), compared to their TSI levels (9.53 ± 12.10 IU/L) with a higher-than-average CAS (2.47 ± 1.78; range, 0-5). Within 12 months of diagnosis, a significant positive correlation between CAS and TRAb (rho = 0.503, p < 0.01) as well as between CAS and TSI (rho = 0.329, p < 0.01) were found. In patients with a diagnosis over 12 months, the correlation with CAS for both TSI and TRAb were Spearman rank correlation coefficient of 0.347 (p < 0.01) and 0.327 (p < 0.01), respectively.</p><p><strong>Conclusions: </strong>TRAb and TSI correlate strongly and to a lesser extent with the CAS. For most patients, TRAb can be replaced with the more economical TSI. TRAb also correlates better with newly diagnosed, more active patients than TSI. In a subset of patients, blocking antibodies may play a significant pathogenic role, requiring different treatment and monitoring. Further studies are required to investigate this relationship.</p>","PeriodicalId":17883,"journal":{"name":"Korean Journal of Ophthalmology : KJO","volume":"37 2","pages":"147-156"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4c/7d/kjo-2022-0131.PMC10151161.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Ophthalmology : KJO","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3341/kjo.2022.0131","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Thyroid receptor antibodies can quantify thyroid eye disease activity, predict outcomes and aid timing of interventions. The type and generation of assay is frequently unspecified, complicating meta-analyses. To determine the clinical and biochemical relationships between a second-generation thyrotropin receptor-binding inhibition antibody (TRAb) immunoassay, detecting stimulatory and blocking antibodies, with the thyroid stimulating immunoglobulin (TSI) bridging immunoassay detecting the stimulatory component only.
Methods: Retrospective review of 100 consecutive patients attending a regional specialist service. For each patient and visit, both a TRAb and TSI were performed, and a clinical activity score (CAS) recorded.
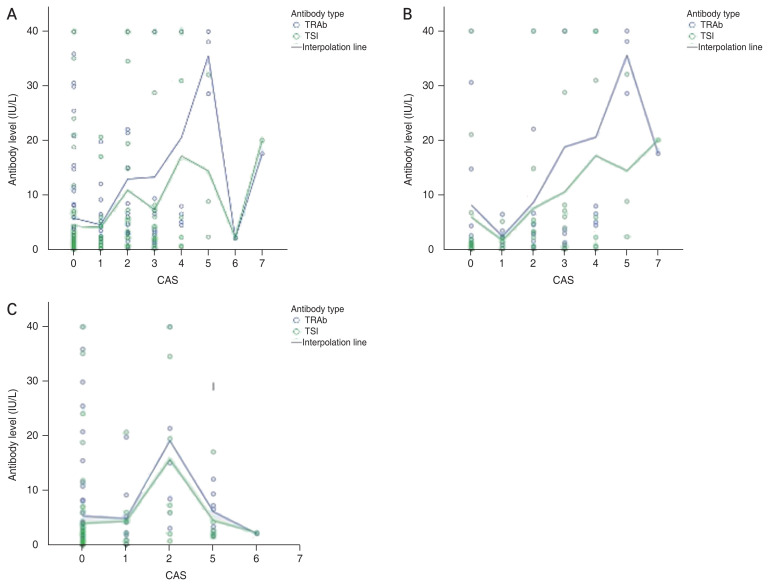
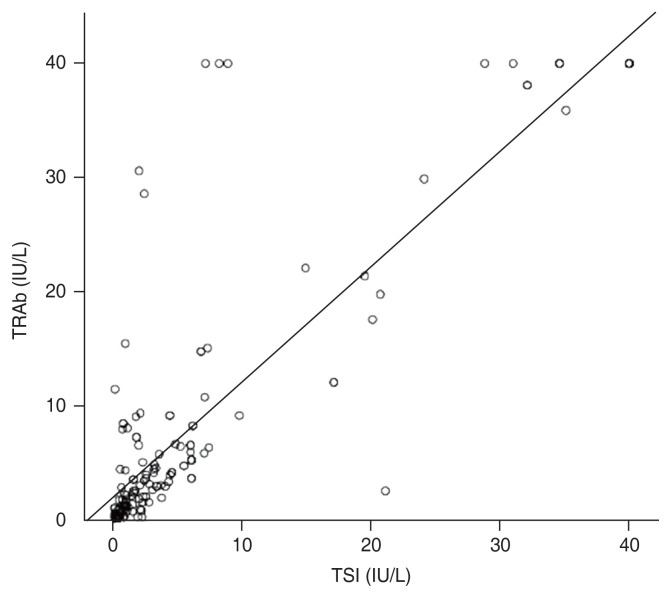
Results: A significant positive correlation between TRAb and TSI (rho = 0.828, p < 0.01) but a weaker correlation between the assays and CAS (TRAb: rho = 0.439, p < 0.01; TSI: r = 0.357, p < 0.01) were found. In 10% of the episodic data, patients had a TRAb level that was disproportionately high (39.41 ± 52.84 IU/L), compared to their TSI levels (9.53 ± 12.10 IU/L) with a higher-than-average CAS (2.47 ± 1.78; range, 0-5). Within 12 months of diagnosis, a significant positive correlation between CAS and TRAb (rho = 0.503, p < 0.01) as well as between CAS and TSI (rho = 0.329, p < 0.01) were found. In patients with a diagnosis over 12 months, the correlation with CAS for both TSI and TRAb were Spearman rank correlation coefficient of 0.347 (p < 0.01) and 0.327 (p < 0.01), respectively.
Conclusions: TRAb and TSI correlate strongly and to a lesser extent with the CAS. For most patients, TRAb can be replaced with the more economical TSI. TRAb also correlates better with newly diagnosed, more active patients than TSI. In a subset of patients, blocking antibodies may play a significant pathogenic role, requiring different treatment and monitoring. Further studies are required to investigate this relationship.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


