Lisa Hinton, Karolina Kuberska, Francesca Dakin, Nicola Boydell, Graham Martin, Tim Draycott, Cathy Winter, Richard J McManus, Lucy Chappell, Sanhita Chakrabarti, Elizabeth Howland, Janet Willars, Mary Dixon-Woods
{"title":"A qualitative study of the dynamics of access to remote antenatal care through the lens of candidacy.","authors":"Lisa Hinton, Karolina Kuberska, Francesca Dakin, Nicola Boydell, Graham Martin, Tim Draycott, Cathy Winter, Richard J McManus, Lucy Chappell, Sanhita Chakrabarti, Elizabeth Howland, Janet Willars, Mary Dixon-Woods","doi":"10.1177/13558196231165361","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We aimed to explore the experiences and perspectives of pregnant women, antenatal healthcare professionals, and system leaders to understand the impact of the implementation of remote provision of antenatal care during the COVID-19 pandemic and beyond.</p><p><strong>Methods: </strong>We conducted a qualitative study involving semi-structured interviews with 93 participants, including 45 individuals who had been pregnant during the study period, 34 health care professionals, and 14 managers and system-level stakeholders. Analysis was based on the constant comparative method and used the theoretical framework of candidacy.</p><p><strong>Results: </strong>We found that remote antenatal care had far-reaching effects on access when understood through the lens of candidacy. It altered women's own identification of themselves and their babies as eligible for antenatal care. Navigating services became more challenging, often requiring considerable digital literacy and sociocultural capital. Services became less permeable, meaning that they were more difficult to use and demanding of the personal and social resources of users. Remote consultations were seen as more transactional in character and were limited by lack of face-to-face contact and safe spaces, making it more difficult for women to make their needs - both clinical and social - known, and for professionals to assess them. Operational and institutional challenges, including problems in sharing of antenatal records, were consequential. There were suggestions that a shift to remote provision of antenatal care might increase risks of inequities in access to care in relation to every feature of candidacy we characterised.</p><p><strong>Conclusion: </strong>It is important to recognise the implications for access to antenatal care of a shift to remote delivery. It is not a simple swap: it restructures many aspects of candidacy for care in ways that pose risks of amplifying existing intersectional inequalities that lead to poorer outcomes. Addressing these challenges through policy and practice action is needed to tackle these risks.</p>","PeriodicalId":15953,"journal":{"name":"Journal of Health Services Research & Policy","volume":" ","pages":"222-232"},"PeriodicalIF":2.7000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10515462/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Services Research & Policy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/13558196231165361","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 2
Abstract
Objective: We aimed to explore the experiences and perspectives of pregnant women, antenatal healthcare professionals, and system leaders to understand the impact of the implementation of remote provision of antenatal care during the COVID-19 pandemic and beyond.
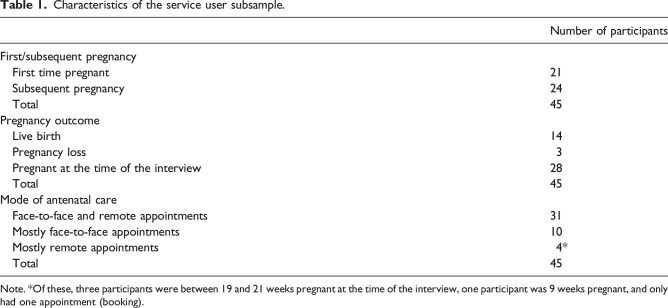
Methods: We conducted a qualitative study involving semi-structured interviews with 93 participants, including 45 individuals who had been pregnant during the study period, 34 health care professionals, and 14 managers and system-level stakeholders. Analysis was based on the constant comparative method and used the theoretical framework of candidacy.
Results: We found that remote antenatal care had far-reaching effects on access when understood through the lens of candidacy. It altered women's own identification of themselves and their babies as eligible for antenatal care. Navigating services became more challenging, often requiring considerable digital literacy and sociocultural capital. Services became less permeable, meaning that they were more difficult to use and demanding of the personal and social resources of users. Remote consultations were seen as more transactional in character and were limited by lack of face-to-face contact and safe spaces, making it more difficult for women to make their needs - both clinical and social - known, and for professionals to assess them. Operational and institutional challenges, including problems in sharing of antenatal records, were consequential. There were suggestions that a shift to remote provision of antenatal care might increase risks of inequities in access to care in relation to every feature of candidacy we characterised.
Conclusion: It is important to recognise the implications for access to antenatal care of a shift to remote delivery. It is not a simple swap: it restructures many aspects of candidacy for care in ways that pose risks of amplifying existing intersectional inequalities that lead to poorer outcomes. Addressing these challenges through policy and practice action is needed to tackle these risks.
期刊介绍:
Journal of Health Services Research & Policy provides a unique opportunity to explore the ideas, policies and decisions shaping health services throughout the world. Edited and peer-reviewed by experts in the field and with a high academic standard and multidisciplinary approach, readers will gain a greater understanding of the current issues in healthcare policy and research. The journal"s strong international editorial advisory board also ensures that readers obtain a truly global and insightful perspective.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


