Juan Luis Gutiérrez-Chico, Carlos Cortés, Mohamed Ayoub, Bernward Lauer, Sylvia Otto, Bernd Reisbeck, Manuela Reisbeck, Christian Schulze, Kambis Mashayekhi
{"title":"Subintimal shift as mechanism for side-branch occlusion in percutaneous treatment of chronic total occlusions with bifurcation lesions.","authors":"Juan Luis Gutiérrez-Chico, Carlos Cortés, Mohamed Ayoub, Bernward Lauer, Sylvia Otto, Bernd Reisbeck, Manuela Reisbeck, Christian Schulze, Kambis Mashayekhi","doi":"10.5603/CJ.a2021.0079","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of this study was to describe the mechanism of subintimal shift (SIS), standardise diagnostic criteria and sensitise the interventional community to this phenomenon. The treatment of chronic total occlusions (CTO) by means of percutaneous coronary intervention (PCI) is complicated by bifurcation lesions involved in the CTO segment or adjacent to it. Extraplaque expansion of intracoronary devices during CTO PCI may extend the dissection plane over the bifurcation with the consequential side or main branch compression by an intimo-medial flap. This phenomenon is hereby described for the first time and named subintimal shift.</p><p><strong>Methods: </strong>Experienced CTO operators from 3 international high volume centers for CTO PCI retrospectively searched their personal records for paradigmatic cases of SIS, summarising key features and proposing diagnostic criteria.</p><p><strong>Results: </strong>The series comprised 7 demonstrative cases, illustrating SIS by intravascular imaging (2 cases) or indirect angiographic signs during CTO PCI (5 cases). Five cases were triggered by stent expansion, 1 by balloon inflation and 1 case was aborted after angiographic warning signs. In 4 cases, SIS resulted in total occlusion of a branch, refractory to ballooning whenever attempted. Four cases required bailout intervention and in 2 cases the branch was left occluded, resulting in a rise of cardiac markers.</p><p><strong>Conclusions: </strong>Subintimal shift is a noteworthy complication in CTO bifurcations, potentially resulting in occlusion of the relevant side or even the main branch. Intracoronary imaging prior to stenting is recommended to understand the tissue planes. Some counterintuitive peculiarities of this phenomenon, like its refractoriness to ballooning, must be known by CTO operators for its efficient resolution.</p>","PeriodicalId":9492,"journal":{"name":"Cardiology journal","volume":"30 1","pages":"24-35"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f5/4a/cardj-30-1-24.PMC9987534.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5603/CJ.a2021.0079","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 5
Abstract
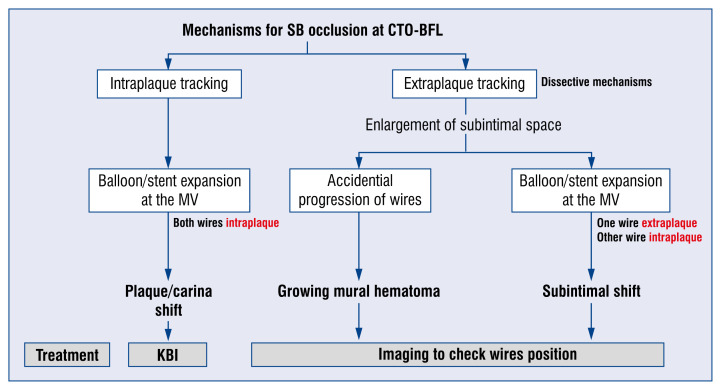
Background: The aim of this study was to describe the mechanism of subintimal shift (SIS), standardise diagnostic criteria and sensitise the interventional community to this phenomenon. The treatment of chronic total occlusions (CTO) by means of percutaneous coronary intervention (PCI) is complicated by bifurcation lesions involved in the CTO segment or adjacent to it. Extraplaque expansion of intracoronary devices during CTO PCI may extend the dissection plane over the bifurcation with the consequential side or main branch compression by an intimo-medial flap. This phenomenon is hereby described for the first time and named subintimal shift.
Methods: Experienced CTO operators from 3 international high volume centers for CTO PCI retrospectively searched their personal records for paradigmatic cases of SIS, summarising key features and proposing diagnostic criteria.
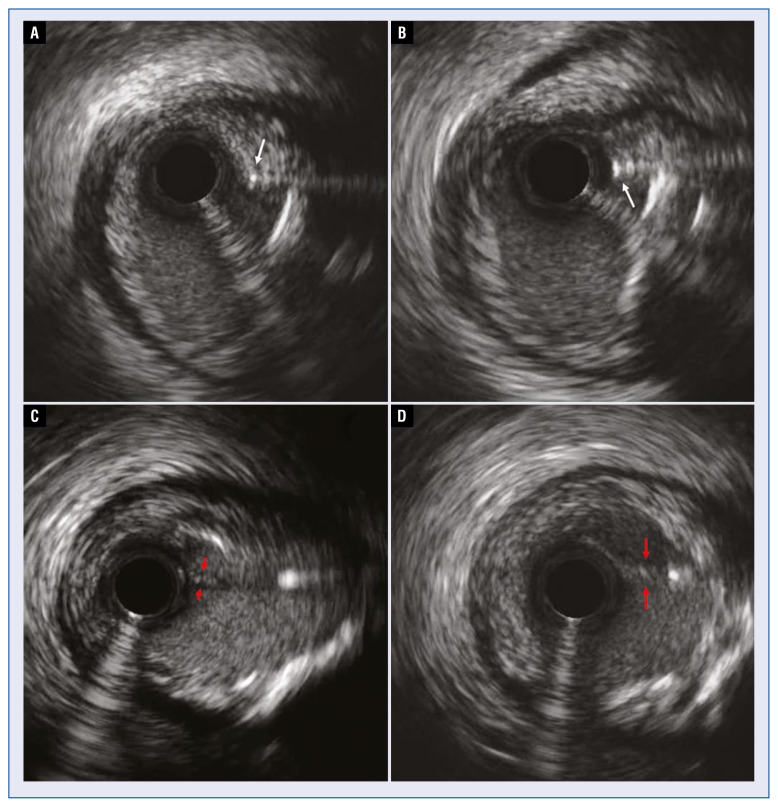
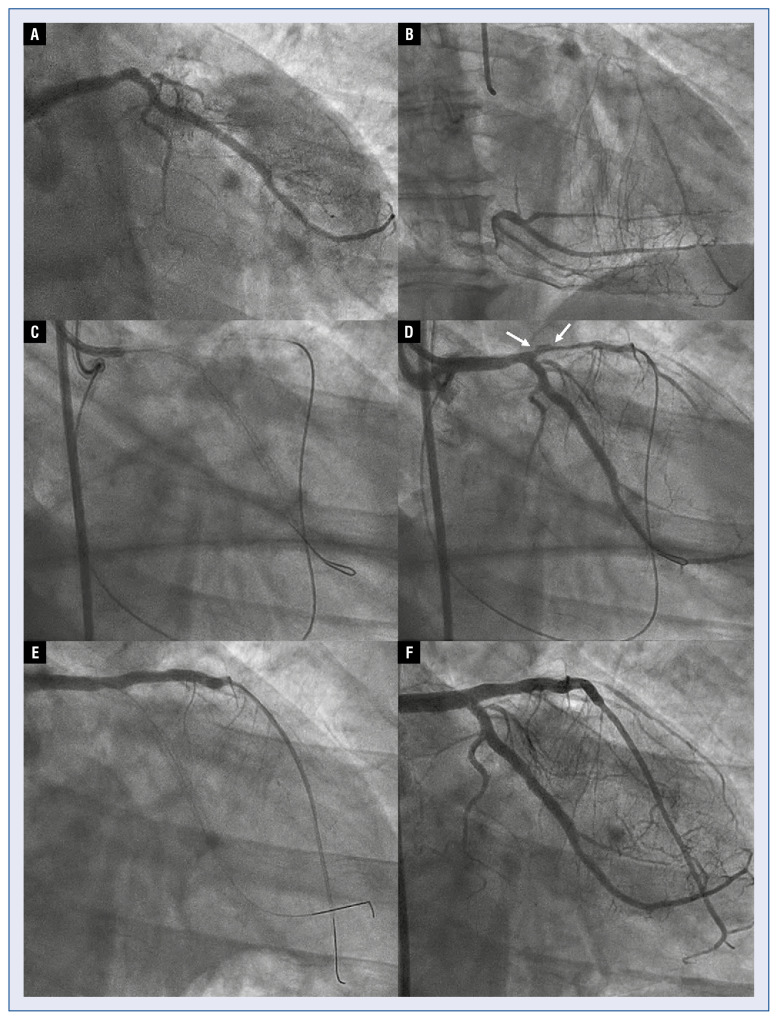
Results: The series comprised 7 demonstrative cases, illustrating SIS by intravascular imaging (2 cases) or indirect angiographic signs during CTO PCI (5 cases). Five cases were triggered by stent expansion, 1 by balloon inflation and 1 case was aborted after angiographic warning signs. In 4 cases, SIS resulted in total occlusion of a branch, refractory to ballooning whenever attempted. Four cases required bailout intervention and in 2 cases the branch was left occluded, resulting in a rise of cardiac markers.
Conclusions: Subintimal shift is a noteworthy complication in CTO bifurcations, potentially resulting in occlusion of the relevant side or even the main branch. Intracoronary imaging prior to stenting is recommended to understand the tissue planes. Some counterintuitive peculiarities of this phenomenon, like its refractoriness to ballooning, must be known by CTO operators for its efficient resolution.
期刊介绍:
Cardiology Journal is a scientific, peer-reviewed journal covering a broad spectrum of topics in cardiology. The journal has been published since 1994 and over the years it has become an internationally recognized journal of cardiological and medical community.
Cardiology Journal is the journal for practicing cardiologists, researchers, and young trainees benefiting from broad spectrum of useful educational content.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


