Shannon Dorsey, Christopher F Akiba, Noah S Triplett, Leah Lucid, Haley A Carroll, Katherine S Benjamin, Dafrosa K Itemba, Augustine I Wasonga, Rachel Manongi, Prerna Martin, Zhanxiang Sun, Kathryn Whetten
{"title":"Consumer perspectives on acceptability of trauma-focused cognitive behavioral therapy in Tanzania and Kenya: A mixed methods study.","authors":"Shannon Dorsey, Christopher F Akiba, Noah S Triplett, Leah Lucid, Haley A Carroll, Katherine S Benjamin, Dafrosa K Itemba, Augustine I Wasonga, Rachel Manongi, Prerna Martin, Zhanxiang Sun, Kathryn Whetten","doi":"10.1177/26334895221109963","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is a substantial mental health treatment gap globally. Increasingly, mental health treatments with evidence of effectiveness in western countries have been adapted and tested in culturally and contextually distinct countries. Findings from these studies have been promising, but to better understand treatment outcome results and consider broader scale up, treatment acceptability needs to be assessed and better understood. This mixed methods study aimed to examine child and guardian acceptability of trauma-focused cognitive behavioral therapy (TF-CBT) in two regions in Tanzania and Kenya and to better understand how TF-CBT was perceived as helpful for children and guardians.</p><p><strong>Methods: </strong>Participants were 315 children (7-13), who experienced the death of one or both parents and 315 guardians, both of whom participated in TF-CBT as part of a randomized controlled trial conducted in Tanzania and Kenya. The study used mixed methods, with quantitative evaluation from guardian perspective (<i>N</i>=315) using the Treatment Acceptability Questionnaire (TAQ) and the Client Satisfaction Questionnaire-8 (CSQ-8). Acceptability was assessed qualitatively from both guardian and child perspectives. Qualitative evaluation involved analysis using stratified selection to identify 160 child and 160 guardian interviews, to allow exploration of potential differences in acceptability by country, setting (urban/rural), and youth age (younger/older).</p><p><strong>Results: </strong>Guardians reported high acceptability on the TAQ and, using an interpretation guide from U.S.-based work, medium acceptability on the CSQ-8. Guardians and children noted high acceptability in the qualitative analysis, noting benefits that correspond to TF-CBT's therapeutic goals. Analyses exploring differences in acceptability yielded few differences by setting or child age but suggested some potential differences by country.</p><p><strong>Conclusion: </strong>Quantitative and qualitative data converged to suggest high acceptability of TF-CBT from guardian and child perspectives in Tanzania and Kenya. Findings add to accumulating evidence of high TF-CBT acceptability from Zambia and other countries (United States, Norway, Australia).<b>Plain Language Summary:</b> Evidence-based treatments have been shown to be effective in countries and regions that are contextually and culturally distinct from where they were developed. But, perspectives of consumers on these treatments have not been assessed regularly or thoroughly. We used open-ended questions and rating scales to assess guardian and youth perspectives on a group-based, cognitive behavioral treatment for children impacted by parental death, in regions within Tanzania and Kenya. Our findings indicate that both guardians and youth found the treatment to be very acceptable. Nearly all guardians talked about specific benefits for the child, followed by benefits for the family and themselves. Eighty percent of youth mentioned benefits for themselves and all youth said they would recommend the program to others. Benefits mentioned by guardians and youth corresponded to treatment goals (improved mood/feelings or behavior, less distress when thinking about the parent/s' death). Both guardians and children named specific aspects of the treatment that they liked and found useful. Dislikes and challenges of the treatment were less frequently mentioned, but point to areas where acceptability could be further improved. Recommendations from participants also offer areas where acceptability could be improved, namely guardians' recommendation that the treatment also address non-mental health needs and offer some follow-up or opportunity to participate in the program again. Our study provides an example of how to assess acceptability and identify places to further enhance acceptability.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"3 ","pages":"26334895221109963"},"PeriodicalIF":2.6000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/71/23/10.1177_26334895221109963.PMC9924250.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895221109963","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: There is a substantial mental health treatment gap globally. Increasingly, mental health treatments with evidence of effectiveness in western countries have been adapted and tested in culturally and contextually distinct countries. Findings from these studies have been promising, but to better understand treatment outcome results and consider broader scale up, treatment acceptability needs to be assessed and better understood. This mixed methods study aimed to examine child and guardian acceptability of trauma-focused cognitive behavioral therapy (TF-CBT) in two regions in Tanzania and Kenya and to better understand how TF-CBT was perceived as helpful for children and guardians.
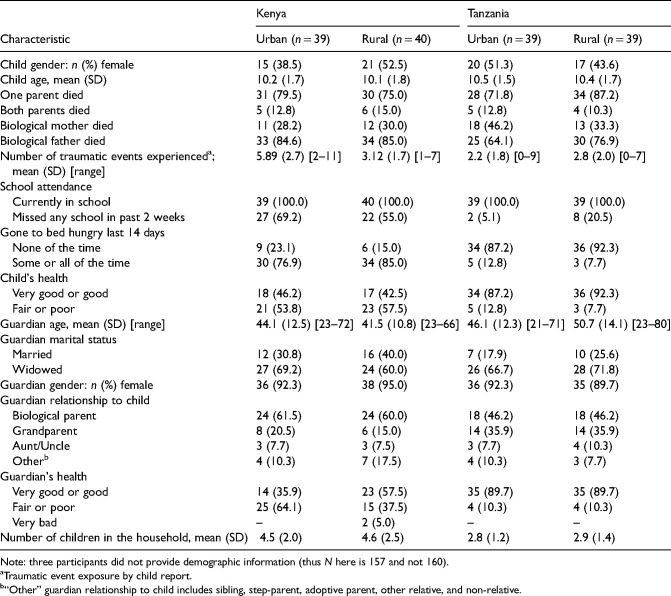
Methods: Participants were 315 children (7-13), who experienced the death of one or both parents and 315 guardians, both of whom participated in TF-CBT as part of a randomized controlled trial conducted in Tanzania and Kenya. The study used mixed methods, with quantitative evaluation from guardian perspective (N=315) using the Treatment Acceptability Questionnaire (TAQ) and the Client Satisfaction Questionnaire-8 (CSQ-8). Acceptability was assessed qualitatively from both guardian and child perspectives. Qualitative evaluation involved analysis using stratified selection to identify 160 child and 160 guardian interviews, to allow exploration of potential differences in acceptability by country, setting (urban/rural), and youth age (younger/older).
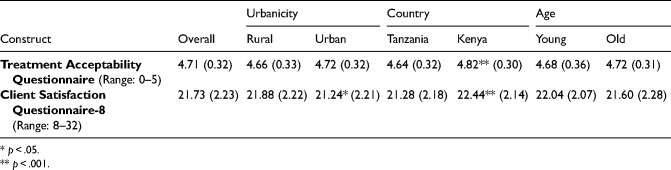
Results: Guardians reported high acceptability on the TAQ and, using an interpretation guide from U.S.-based work, medium acceptability on the CSQ-8. Guardians and children noted high acceptability in the qualitative analysis, noting benefits that correspond to TF-CBT's therapeutic goals. Analyses exploring differences in acceptability yielded few differences by setting or child age but suggested some potential differences by country.
Conclusion: Quantitative and qualitative data converged to suggest high acceptability of TF-CBT from guardian and child perspectives in Tanzania and Kenya. Findings add to accumulating evidence of high TF-CBT acceptability from Zambia and other countries (United States, Norway, Australia).Plain Language Summary: Evidence-based treatments have been shown to be effective in countries and regions that are contextually and culturally distinct from where they were developed. But, perspectives of consumers on these treatments have not been assessed regularly or thoroughly. We used open-ended questions and rating scales to assess guardian and youth perspectives on a group-based, cognitive behavioral treatment for children impacted by parental death, in regions within Tanzania and Kenya. Our findings indicate that both guardians and youth found the treatment to be very acceptable. Nearly all guardians talked about specific benefits for the child, followed by benefits for the family and themselves. Eighty percent of youth mentioned benefits for themselves and all youth said they would recommend the program to others. Benefits mentioned by guardians and youth corresponded to treatment goals (improved mood/feelings or behavior, less distress when thinking about the parent/s' death). Both guardians and children named specific aspects of the treatment that they liked and found useful. Dislikes and challenges of the treatment were less frequently mentioned, but point to areas where acceptability could be further improved. Recommendations from participants also offer areas where acceptability could be improved, namely guardians' recommendation that the treatment also address non-mental health needs and offer some follow-up or opportunity to participate in the program again. Our study provides an example of how to assess acceptability and identify places to further enhance acceptability.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


