Edwin S Wong, Suparna Rajan, Chuan-Fen Liu, Leslie A Morland, Jeffrey M Pyne, Fatma Simsek-Duran, Heather S Reisinger, Jane Moeckli, John C Fortney
{"title":"Economic costs of implementing evidence-based telemedicine outreach for posttraumatic stress disorder in VA.","authors":"Edwin S Wong, Suparna Rajan, Chuan-Fen Liu, Leslie A Morland, Jeffrey M Pyne, Fatma Simsek-Duran, Heather S Reisinger, Jane Moeckli, John C Fortney","doi":"10.1177/26334895221116771","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Telemedicine outreach for posttraumatic stress disorder (TOP) is a virtual evidence-based practice (EBP) involving telephone care management and telepsychology that engages rural patients in trauma-focused psychotherapy. This evaluation examined implementation and intervention costs attributable to deploying TOP from a health system perspective.</p><p><strong>Methods: </strong>Costs were ascertained as part of a stepped wedge cluster randomized trial at five sites within the Veterans Affairs (VA) Healthcare System. All sites initially received a <i>standard implementation</i> strategy, which included internal facilitation, dissemination of an internal facilitators operational guide, funded care manager, care managing training, and technical support. A subset of clinics that failed to meet performance metrics were subsequently randomized to <i>enhanced implementation</i>, which added external facilitation that focused on incorporating TOP clinical processes into existing clinic workflow. We measured site-level implementation activities using project records and structured activity logs tracking personnel-level time devoted to all implementation activities. We monetized time devoted to implementation activities by applying an opportunity cost approach. Intervention costs were measured as accounting-based costs for telepsychiatry/telepsychology and care manager visits, ascertained using VA administrative data. We conducted descriptive analyses of strategy-specific implementation costs across five sites. Descriptive analyses were conducted instead of population-level cost-effectiveness analysis because previous research found enhanced implementation was not more successful than the standard implementation in improving uptake of TOP.</p><p><strong>Results: </strong>Over the 40-month study period, four of five sites received enhanced implementation. Mean site-level implementation cost per month was $919 (SD = $238) during standard implementation and increased to $1,651 (SD = $460) during enhanced implementation. Mean site-level intervention cost per patient-month was $46 (SD = $28) during standard implementation and $31 (SD = $21) during enhanced implementation.</p><p><strong>Conclusions: </strong>Project findings inform the expected cost of implementing TOP, which represents one factor health systems should consider in the decision to broadly adopt this EBP. <b>Plain Language Summary:</b> <i>What is already known about the topic:</i> Trauma-focused psychotherapy delivered through telemedicine has been demonstrated as an effective approach for the treatment of post-traumatic stress disorder (PTSD). However, uptake of this evidence-based approach by integrated health systems such as the Veterans Affairs (VA) Health Care System is low. <i>What does this paper add:</i> This paper presents new findings on the costs of two implementation approaches designed to increase adoption telemedicine outreach for PTSD from a health system perspective. <i>What are the implications for practice, research, and policy:</i> Cost estimates from this paper can be used by health systems to inform the relative value of candidate implementation strategies to increase adoption of evidence-based treatments for PTSD or other mental health conditions.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"3 ","pages":"26334895221116771"},"PeriodicalIF":2.6000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9c/84/10.1177_26334895221116771.PMC9924252.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895221116771","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Telemedicine outreach for posttraumatic stress disorder (TOP) is a virtual evidence-based practice (EBP) involving telephone care management and telepsychology that engages rural patients in trauma-focused psychotherapy. This evaluation examined implementation and intervention costs attributable to deploying TOP from a health system perspective.
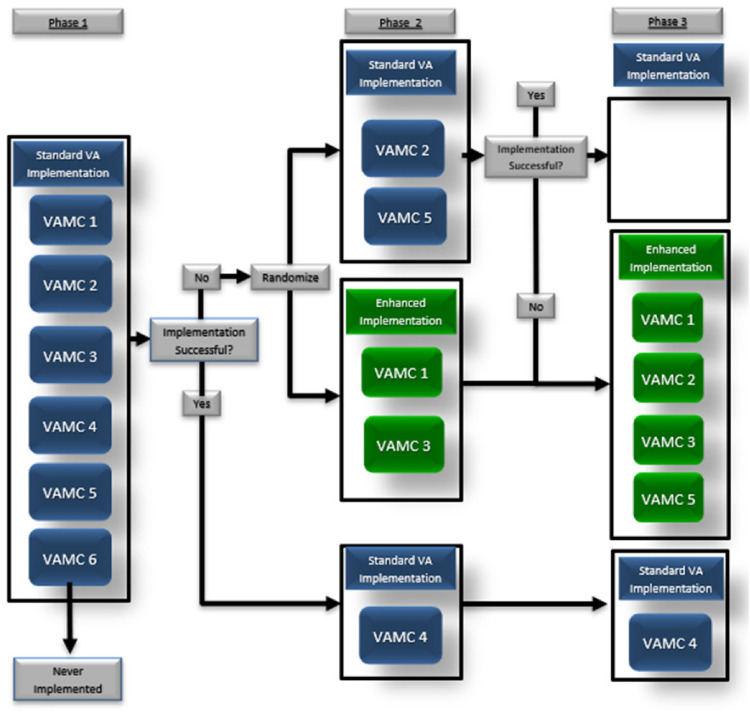
Methods: Costs were ascertained as part of a stepped wedge cluster randomized trial at five sites within the Veterans Affairs (VA) Healthcare System. All sites initially received a standard implementation strategy, which included internal facilitation, dissemination of an internal facilitators operational guide, funded care manager, care managing training, and technical support. A subset of clinics that failed to meet performance metrics were subsequently randomized to enhanced implementation, which added external facilitation that focused on incorporating TOP clinical processes into existing clinic workflow. We measured site-level implementation activities using project records and structured activity logs tracking personnel-level time devoted to all implementation activities. We monetized time devoted to implementation activities by applying an opportunity cost approach. Intervention costs were measured as accounting-based costs for telepsychiatry/telepsychology and care manager visits, ascertained using VA administrative data. We conducted descriptive analyses of strategy-specific implementation costs across five sites. Descriptive analyses were conducted instead of population-level cost-effectiveness analysis because previous research found enhanced implementation was not more successful than the standard implementation in improving uptake of TOP.
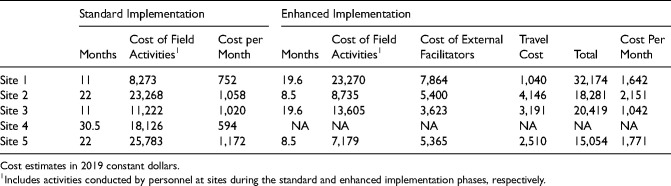
Results: Over the 40-month study period, four of five sites received enhanced implementation. Mean site-level implementation cost per month was $919 (SD = $238) during standard implementation and increased to $1,651 (SD = $460) during enhanced implementation. Mean site-level intervention cost per patient-month was $46 (SD = $28) during standard implementation and $31 (SD = $21) during enhanced implementation.
Conclusions: Project findings inform the expected cost of implementing TOP, which represents one factor health systems should consider in the decision to broadly adopt this EBP. Plain Language Summary:What is already known about the topic: Trauma-focused psychotherapy delivered through telemedicine has been demonstrated as an effective approach for the treatment of post-traumatic stress disorder (PTSD). However, uptake of this evidence-based approach by integrated health systems such as the Veterans Affairs (VA) Health Care System is low. What does this paper add: This paper presents new findings on the costs of two implementation approaches designed to increase adoption telemedicine outreach for PTSD from a health system perspective. What are the implications for practice, research, and policy: Cost estimates from this paper can be used by health systems to inform the relative value of candidate implementation strategies to increase adoption of evidence-based treatments for PTSD or other mental health conditions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


