S M Savarimuthu, C Cairns, N L Allorto, G E Weissman, R Kohn, R D Wise, G L Anesi
{"title":"qSOFA as a predictor of ICU outcomes in a resource-limited setting in KwaZulu-Natal Province, South Africa.","authors":"S M Savarimuthu, C Cairns, N L Allorto, G E Weissman, R Kohn, R D Wise, G L Anesi","doi":"10.7196/SAJCC.2020.v36i2.433","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis is a major cause of morbidity and mortality, especially in critical care patients. Developing tools to identify patients who are at risk of poor outcomes and prolonged length of stay in intensive care units (ICUs) is critical, particularly in resource-limited settings.</p><p><strong>Objectives: </strong>To determine whether the quick sequential organ failure assessment (qSOFA) score based on bedside assessment alone was a promising tool for risk prediction in low-resource settings.</p><p><strong>Methods: </strong>A retrospective cohort of adult patients admitted to the intensive care unit (ICU) at Edendale Hospital in Pietermaritzburg, South Africa (SA), was recruited into the study between 2014 and 2018. The association of qSOFA with in-ICU mortality was measured using multivariable logistic regression. Discrimination was assessed using the area under the receiver operating characteristic curve and the additive contribution to a baseline model using likelihood ratio testing.</p><p><strong>Results: </strong>The qSOFA scores of 0, 1 and 2 were not associated with increased odds of in-ICU mortality (adjusted odds ratio (aOR) 1.24, 95% confidence interval (CI) 0.86 - 1.79; <i>p</i>=0.26) in patients with infection, while the qSOFA of 3 was associated with in-ICU mortality in infected patients (aOR 2.82; 95% CI 1.91 - 4.16; <i>p</i><0.001). On the other hand, the qSOFA scores of 2 (aOR 3.25; 95% CI 1.91 - 5.53; <i>p</i><0.001) and 3 (aOR 6.26, 95% CI 0.38 - 11.62, <i>p</i><0.001) were associated with increased odds of in-ICU mortality in patients without infection. Discrimination for mortality was fair to poor and adding qSOFA to a baseline model yielded a statistical improvement in both cases (<i>p</i><0.001).</p><p><strong>Conclusion: </strong>qSOFA was associated with, but weakly discriminant, for in-ICU mortality for patients with and without infection in a resource-limited, public hospital in SA. These findings add to the growing body of evidence that support the use of qSOFA to deliver low-cost, high-value critical care in resource-limited settings.</p><p><strong>Contributions of the study: </strong>This study expanded the data supporting the use of qSOFA in resource-limited settings beyond the emergency department or ward to include patients admitted to the ICU. Additionally, this study demonstrated stronger predictive abilities in a population of patients admitted with trauma without suspected or confirmed infection, thus providing an additional use of qSOFA as a risk-prediction tool for a broader population.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":"36 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/9f/SAJCC-36-2-433.PMC9045512.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2020.v36i2.433","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
Background: Sepsis is a major cause of morbidity and mortality, especially in critical care patients. Developing tools to identify patients who are at risk of poor outcomes and prolonged length of stay in intensive care units (ICUs) is critical, particularly in resource-limited settings.
Objectives: To determine whether the quick sequential organ failure assessment (qSOFA) score based on bedside assessment alone was a promising tool for risk prediction in low-resource settings.
Methods: A retrospective cohort of adult patients admitted to the intensive care unit (ICU) at Edendale Hospital in Pietermaritzburg, South Africa (SA), was recruited into the study between 2014 and 2018. The association of qSOFA with in-ICU mortality was measured using multivariable logistic regression. Discrimination was assessed using the area under the receiver operating characteristic curve and the additive contribution to a baseline model using likelihood ratio testing.
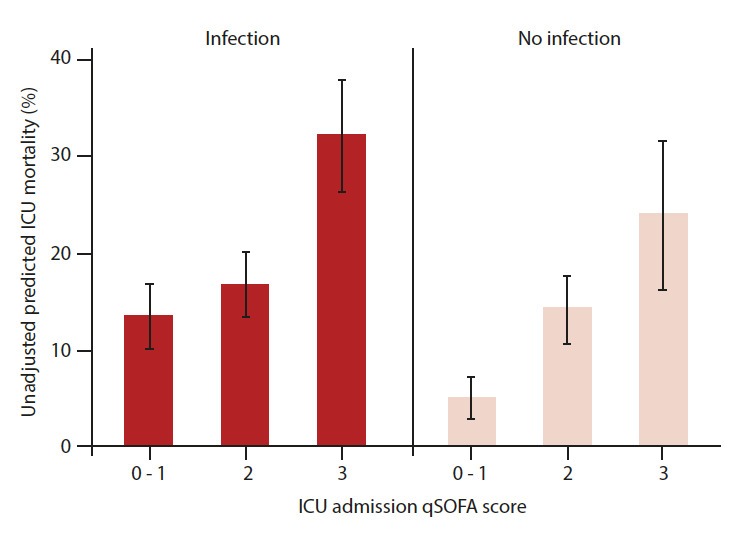
Results: The qSOFA scores of 0, 1 and 2 were not associated with increased odds of in-ICU mortality (adjusted odds ratio (aOR) 1.24, 95% confidence interval (CI) 0.86 - 1.79; p=0.26) in patients with infection, while the qSOFA of 3 was associated with in-ICU mortality in infected patients (aOR 2.82; 95% CI 1.91 - 4.16; p<0.001). On the other hand, the qSOFA scores of 2 (aOR 3.25; 95% CI 1.91 - 5.53; p<0.001) and 3 (aOR 6.26, 95% CI 0.38 - 11.62, p<0.001) were associated with increased odds of in-ICU mortality in patients without infection. Discrimination for mortality was fair to poor and adding qSOFA to a baseline model yielded a statistical improvement in both cases (p<0.001).
Conclusion: qSOFA was associated with, but weakly discriminant, for in-ICU mortality for patients with and without infection in a resource-limited, public hospital in SA. These findings add to the growing body of evidence that support the use of qSOFA to deliver low-cost, high-value critical care in resource-limited settings.
Contributions of the study: This study expanded the data supporting the use of qSOFA in resource-limited settings beyond the emergency department or ward to include patients admitted to the ICU. Additionally, this study demonstrated stronger predictive abilities in a population of patients admitted with trauma without suspected or confirmed infection, thus providing an additional use of qSOFA as a risk-prediction tool for a broader population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


