The sensitivity and specificity of using the McGill pain subscale for diagnosing neuropathic and non-neuropathic chronic pain in the total joint arthroplasty population.
Dragana Boljanovic-Susic, Christina Ziebart, Joy MacDermid, Justin de Beer, Danielle Petruccelli, Linda J Woodhouse
{"title":"The sensitivity and specificity of using the McGill pain subscale for diagnosing neuropathic and non-neuropathic chronic pain in the total joint arthroplasty population.","authors":"Dragana Boljanovic-Susic, Christina Ziebart, Joy MacDermid, Justin de Beer, Danielle Petruccelli, Linda J Woodhouse","doi":"10.1186/s40945-023-00164-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The purpose of this study was to describe the diagnostic performance of the Neuropathic Pain Subscale of McGill [NP-MPQ (SF-2)] and the Self-Administered Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) questionnaire in differentiating people with neuropathic chronic pain post total joint arthroplasty (TJA).</p><p><strong>Methods: </strong>This study was a survey of a cohort of individuals who had undergone primary, unilateral total knee, or hip joint arthroplasty. The questionnaires were administered by mail. The time interval from operation to the completion of the postal survey varied from 1.5 to 3.5 years post-surgery. Receiver Operating Characteristic (ROC) analysis was used to assess the overall diagnostic power and determine the optimal threshold value of the NP-MPQ (SF-2) in identification of neuropathic pain.</p><p><strong>Results: </strong>S-LANSS identified 19 subjects (28%) as having neuropathic pain (NP), while NP-MPQ (SF-2) subscale identified 29 (43%). When using the S-LANSS as the reference standard, a Receiver Operating Characteristic (ROC) analysis for NP-MPQ (SF-2) had an area under the curve of 0.89 (95% CI: 0.82, 0.97); a cut off score of 0.91 NP-MPQ (SF-2) maximized sensitivity (89.5%) and specificity (75.0%). Correlation between the measures was moderate (r = 0.56; 95% CI: 0.40, 0.68).</p><p><strong>Conclusion: </strong>These finding suggest some conceptual overlap but some variability in diagnosis of NP which may relate to scale-tapping into different dimensions of the pain experience, or the different scoring metrics.</p>","PeriodicalId":72290,"journal":{"name":"Archives of physiotherapy","volume":"13 1","pages":"9"},"PeriodicalIF":2.1000,"publicationDate":"2023-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10127094/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of physiotherapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40945-023-00164-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The purpose of this study was to describe the diagnostic performance of the Neuropathic Pain Subscale of McGill [NP-MPQ (SF-2)] and the Self-Administered Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) questionnaire in differentiating people with neuropathic chronic pain post total joint arthroplasty (TJA).
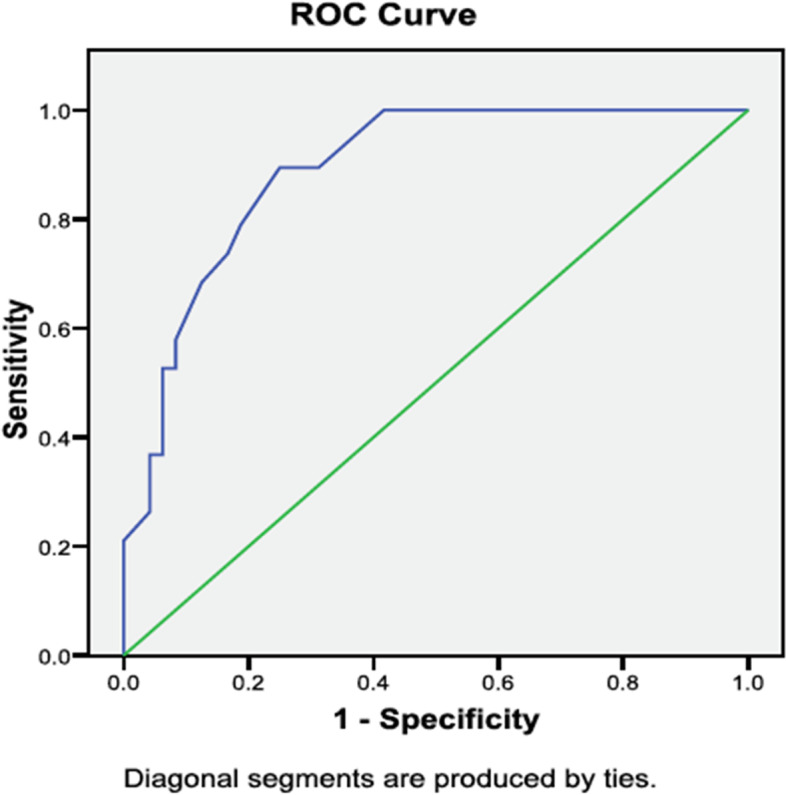
Methods: This study was a survey of a cohort of individuals who had undergone primary, unilateral total knee, or hip joint arthroplasty. The questionnaires were administered by mail. The time interval from operation to the completion of the postal survey varied from 1.5 to 3.5 years post-surgery. Receiver Operating Characteristic (ROC) analysis was used to assess the overall diagnostic power and determine the optimal threshold value of the NP-MPQ (SF-2) in identification of neuropathic pain.
Results: S-LANSS identified 19 subjects (28%) as having neuropathic pain (NP), while NP-MPQ (SF-2) subscale identified 29 (43%). When using the S-LANSS as the reference standard, a Receiver Operating Characteristic (ROC) analysis for NP-MPQ (SF-2) had an area under the curve of 0.89 (95% CI: 0.82, 0.97); a cut off score of 0.91 NP-MPQ (SF-2) maximized sensitivity (89.5%) and specificity (75.0%). Correlation between the measures was moderate (r = 0.56; 95% CI: 0.40, 0.68).
Conclusion: These finding suggest some conceptual overlap but some variability in diagnosis of NP which may relate to scale-tapping into different dimensions of the pain experience, or the different scoring metrics.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


