A typology of power in implementation: Building on the exploration, preparation, implementation, sustainment (EPIS) framework to advance mental health and HIV health equity.
Megan C Stanton, Samira B Ali, The Sustain Center Team
{"title":"A typology of power in implementation: Building on the exploration, preparation, implementation, sustainment (EPIS) framework to advance mental health and HIV health equity.","authors":"Megan C Stanton, Samira B Ali, The Sustain Center Team","doi":"10.1177/26334895211064250","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Persistent inequities in HIV health are due, in part, to barriers to successful HIV-related mental health intervention implementation with marginalized groups. Implementation Science (IS) has begun to examine how the field can promote health equity. Lacking is a clear method to analyze how power is generated and distributed through practical implementation processes and how this power can dismantle and/or reproduce health inequity through intervention implementation. The aims of this paper are to (1) propose a typology of power generated through implementation processes, (2) apply this power typology to expand on the Exploration, Preparation, Implementation, Sustainment (EPIS) framework to advance HIV and mental health equity and (3) articulate questions to guide the explicit examination and distribution of power throughout implementation.</p><p><strong>Methods: </strong>This paper draws on the work of an Intermediary Purveyor organization implementing trauma-informed care and harm reduction organizational change with HIV service organizations. The expanded framework was developed through analyzing implementation coaching field notes, grant reporting, and evaluation documents, training feedback, partner evaluation interviews, and existing implementation literature.</p><p><strong>Results: </strong>The authors identify three types of power working through implementation; (1) <b><i>discursive power</i></b> is enacted through defining health-related problems to be targeted by intervention implementation, as well as through health narratives that emerge through implementation; (2) <b><i>epistemic power</i></b> influences whose knowledge is valued in decision-making and is recreated through knowledge generation; and (3) <b><i>material power</i></b> is created through resource distribution and patterns of access to health resources and acquisition of health benefits provided by the intervention. Decisions across all phases and related to all factors of EPIS influence how these forms of power striate through intervention implementation and ultimately affect health equity outcomes.</p><p><strong>Conclusions: </strong>The authors conclude with a set of concrete questions for researchers and practitioners to interrogate power throughout the implementation process.</p><p><strong>Plain language summary: </strong>Over the past few years, Implementation Science researchers have committed increased attention to the ways in which the field can more effectively address health inequity. Lacking is a clear method to analyze how implementation processes themselves generate power that has the potential to contribute to health inequity. In this paper, the authors describe and define three types of power that are created and distributed through intervention implementation; discursive power, epistemic power, and material power. The authors then explain how these forms of power shape factors and phases of implementation, using the well-known EPIS (exploration, preparation, implementation, sustainment) framework. The authors draw from their experience working with and Intermediary Purveyor supporting HIV service organizations implementing trauma-informed care and harm reduction organizational change projects. This paper concludes with a set of critical questions that can be used by researchers and practitioners as a concrete tool to analyze the role of power in intervention implementation processes.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"3 ","pages":"26334895211064250"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/55/1f/10.1177_26334895211064250.PMC9978699.pdf","citationCount":"11","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895211064250","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 11
Abstract
Background: Persistent inequities in HIV health are due, in part, to barriers to successful HIV-related mental health intervention implementation with marginalized groups. Implementation Science (IS) has begun to examine how the field can promote health equity. Lacking is a clear method to analyze how power is generated and distributed through practical implementation processes and how this power can dismantle and/or reproduce health inequity through intervention implementation. The aims of this paper are to (1) propose a typology of power generated through implementation processes, (2) apply this power typology to expand on the Exploration, Preparation, Implementation, Sustainment (EPIS) framework to advance HIV and mental health equity and (3) articulate questions to guide the explicit examination and distribution of power throughout implementation.
Methods: This paper draws on the work of an Intermediary Purveyor organization implementing trauma-informed care and harm reduction organizational change with HIV service organizations. The expanded framework was developed through analyzing implementation coaching field notes, grant reporting, and evaluation documents, training feedback, partner evaluation interviews, and existing implementation literature.
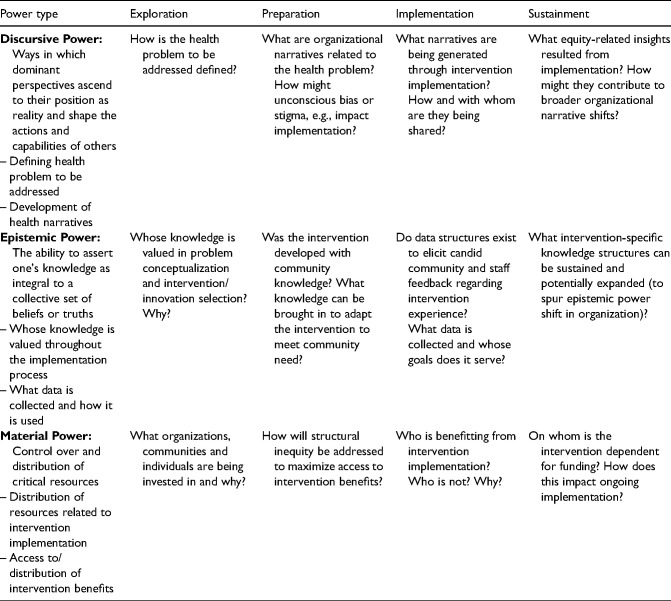
Results: The authors identify three types of power working through implementation; (1) discursive power is enacted through defining health-related problems to be targeted by intervention implementation, as well as through health narratives that emerge through implementation; (2) epistemic power influences whose knowledge is valued in decision-making and is recreated through knowledge generation; and (3) material power is created through resource distribution and patterns of access to health resources and acquisition of health benefits provided by the intervention. Decisions across all phases and related to all factors of EPIS influence how these forms of power striate through intervention implementation and ultimately affect health equity outcomes.
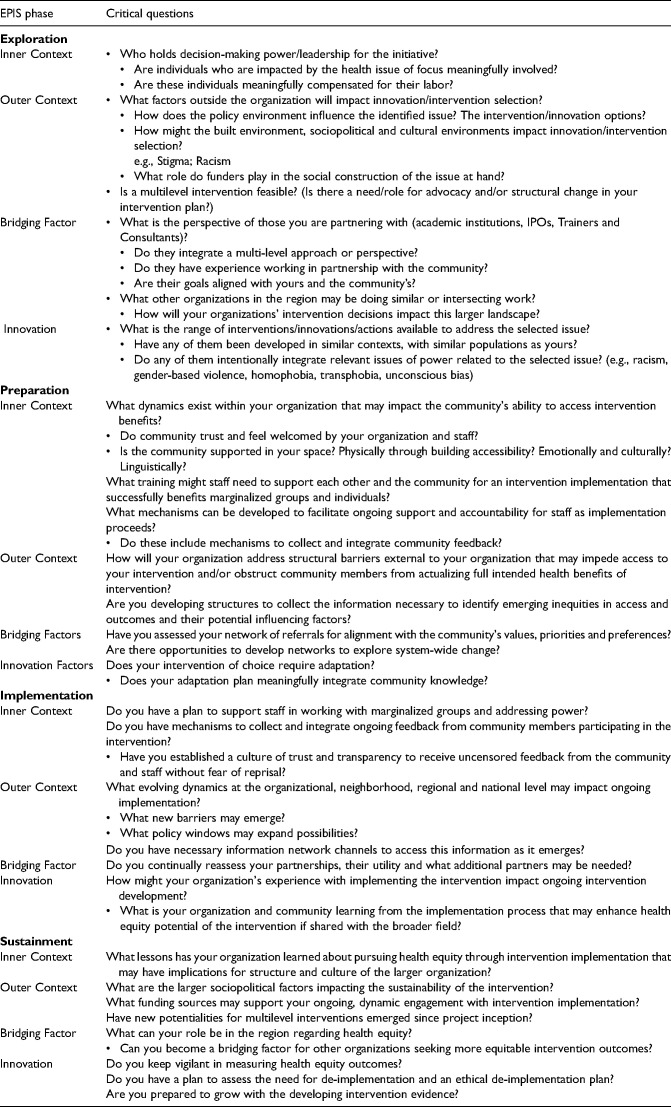
Conclusions: The authors conclude with a set of concrete questions for researchers and practitioners to interrogate power throughout the implementation process.
Plain language summary: Over the past few years, Implementation Science researchers have committed increased attention to the ways in which the field can more effectively address health inequity. Lacking is a clear method to analyze how implementation processes themselves generate power that has the potential to contribute to health inequity. In this paper, the authors describe and define three types of power that are created and distributed through intervention implementation; discursive power, epistemic power, and material power. The authors then explain how these forms of power shape factors and phases of implementation, using the well-known EPIS (exploration, preparation, implementation, sustainment) framework. The authors draw from their experience working with and Intermediary Purveyor supporting HIV service organizations implementing trauma-informed care and harm reduction organizational change projects. This paper concludes with a set of critical questions that can be used by researchers and practitioners as a concrete tool to analyze the role of power in intervention implementation processes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


