Xi Zhang, Aparna Gunda, Elma Meershoek-Klein Kranenbarg, Gerrit-Jan Liefers, Badada Ananthamurthy Savitha, Payal Shrivastava, Chandra Prakash Vijay Kumar Serkad, Taranjot Kaur, Mallikarjuna Siraganahalli Eshwaraiah, Rob A E M Tollenaar, Cornelis J H van de Velde, Caroline M J Seynaeve, Manjiri Bakre, Peter J K Kuppen
{"title":"Ten-year distant-recurrence risk prediction in breast cancer by CanAssist Breast (CAB) in Dutch sub-cohort of the randomized TEAM trial.","authors":"Xi Zhang, Aparna Gunda, Elma Meershoek-Klein Kranenbarg, Gerrit-Jan Liefers, Badada Ananthamurthy Savitha, Payal Shrivastava, Chandra Prakash Vijay Kumar Serkad, Taranjot Kaur, Mallikarjuna Siraganahalli Eshwaraiah, Rob A E M Tollenaar, Cornelis J H van de Velde, Caroline M J Seynaeve, Manjiri Bakre, Peter J K Kuppen","doi":"10.1186/s13058-023-01643-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hormone receptor (HR)-positive, HER2/neu-negative breast cancers have a sustained risk of recurrence up to 20 years from diagnosis. TEAM (Tamoxifen, Exemestane Adjuvant Multinational) is a large, multi-country, phase III trial that randomized 9776 women for the use of hormonal therapy. Of these 2754 were Dutch patients. The current study aims for the first time to correlate the ten-year clinical outcomes with predictions by CanAssist Breast (CAB)-a prognostic test developed in South East Asia, on a Dutch sub-cohort that participated in the TEAM. The total Dutch TEAM cohort and the current Dutch sub-cohort were almost similar with respect to patient age and tumor anatomical features.</p><p><strong>Methods: </strong>Of the 2754 patients from the Netherlands, which are part of the original TEAM trial, 592 patients' samples were available with Leiden University Medical Center (LUMC). The risk stratification of CAB was correlated with outcomes of patients using logistic regression approaches entailing Kaplan-Meier survival curves, univariate and multivariate cox-regression hazards model. We used hazard ratios (HRs), the cumulative incidence of distant metastasis/death due to breast cancer (DM), and distant recurrence-free interval (DRFi) for assessment.</p><p><strong>Results: </strong>Out of 433 patients finally included, the majority, 68.4% had lymph node-positive disease, while only a minority received chemotherapy (20.8%) in addition to endocrine therapy. CAB stratified 67.5% of the total cohort as low-risk [DM = 11.5% (95% CI, 7.6-15.2)] and 32.5% as high-risk [DM = 30.2% (95% CI, 21.9-37.6)] with an HR of 2.90 (95% CI, 1.75-4.80; P < 0.001) at ten years. CAB risk score was an independent prognostic factor in the consideration of clinical parameters in multivariate analysis. At ten years, CAB high-risk had the worst DRFi of 69.8%, CAB low-risk in the exemestane monotherapy arm had the best DRFi of 92.7% [vs CAB high-risk, HR, 0.21 (95% CI, 0.11-0.43), P < 0.001], and CAB low-risk in the sequential arm had a DRFi of 84.2% [vs CAB high-risk, HR, 0.48 (95% CI, 0.28-0.82), P = 0.009].</p><p><strong>Conclusions: </strong>Cost-effective CAB is a statistically robust prognostic and predictive tool for ten-year DM for postmenopausal women with HR+/HER2-, early breast cancer. CAB low-risk patients who received exemestane monotherapy had an excellent ten-year DRFi.</p>","PeriodicalId":9283,"journal":{"name":"Breast Cancer Research : BCR","volume":"25 1","pages":"40"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10103430/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Cancer Research : BCR","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13058-023-01643-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Hormone receptor (HR)-positive, HER2/neu-negative breast cancers have a sustained risk of recurrence up to 20 years from diagnosis. TEAM (Tamoxifen, Exemestane Adjuvant Multinational) is a large, multi-country, phase III trial that randomized 9776 women for the use of hormonal therapy. Of these 2754 were Dutch patients. The current study aims for the first time to correlate the ten-year clinical outcomes with predictions by CanAssist Breast (CAB)-a prognostic test developed in South East Asia, on a Dutch sub-cohort that participated in the TEAM. The total Dutch TEAM cohort and the current Dutch sub-cohort were almost similar with respect to patient age and tumor anatomical features.
Methods: Of the 2754 patients from the Netherlands, which are part of the original TEAM trial, 592 patients' samples were available with Leiden University Medical Center (LUMC). The risk stratification of CAB was correlated with outcomes of patients using logistic regression approaches entailing Kaplan-Meier survival curves, univariate and multivariate cox-regression hazards model. We used hazard ratios (HRs), the cumulative incidence of distant metastasis/death due to breast cancer (DM), and distant recurrence-free interval (DRFi) for assessment.
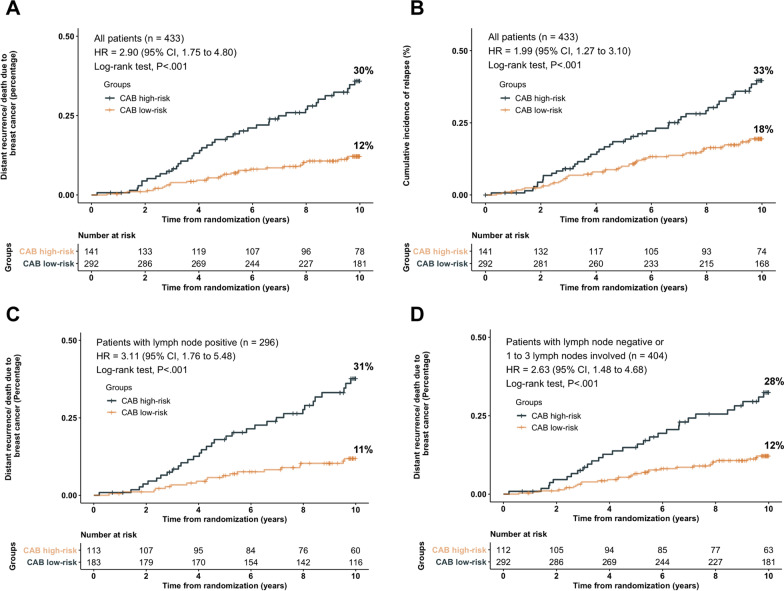
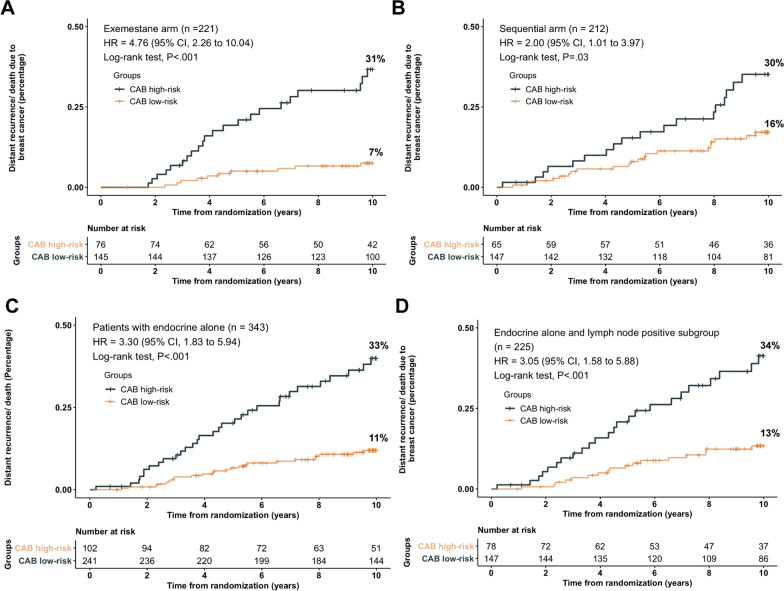
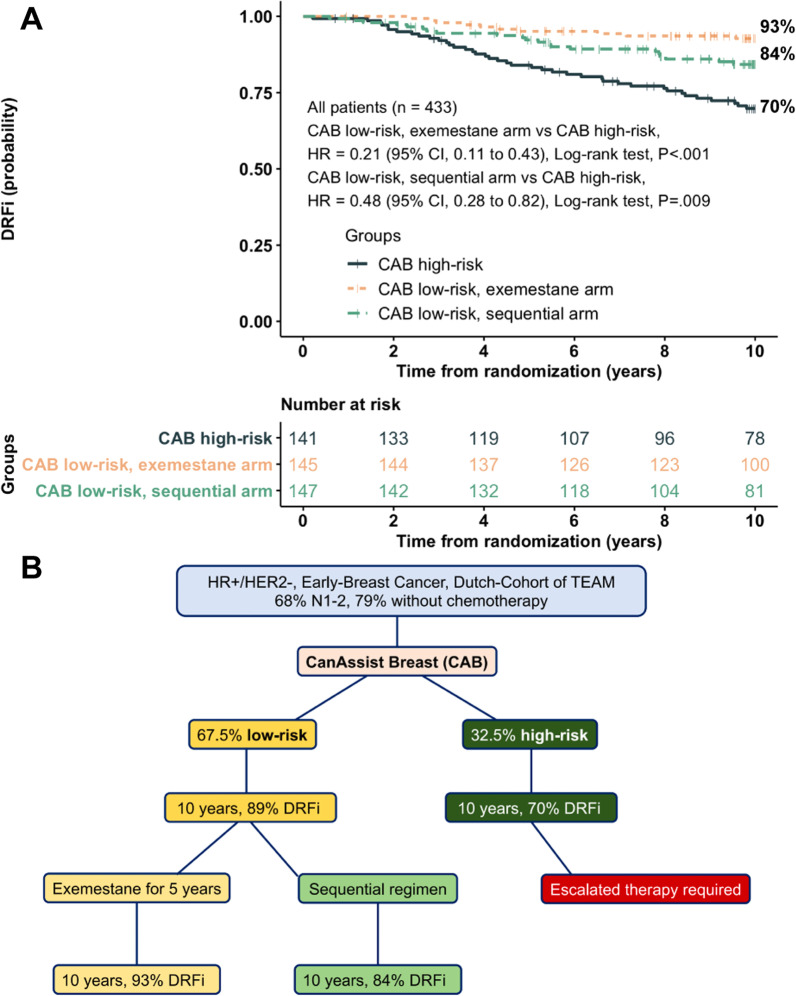
Results: Out of 433 patients finally included, the majority, 68.4% had lymph node-positive disease, while only a minority received chemotherapy (20.8%) in addition to endocrine therapy. CAB stratified 67.5% of the total cohort as low-risk [DM = 11.5% (95% CI, 7.6-15.2)] and 32.5% as high-risk [DM = 30.2% (95% CI, 21.9-37.6)] with an HR of 2.90 (95% CI, 1.75-4.80; P < 0.001) at ten years. CAB risk score was an independent prognostic factor in the consideration of clinical parameters in multivariate analysis. At ten years, CAB high-risk had the worst DRFi of 69.8%, CAB low-risk in the exemestane monotherapy arm had the best DRFi of 92.7% [vs CAB high-risk, HR, 0.21 (95% CI, 0.11-0.43), P < 0.001], and CAB low-risk in the sequential arm had a DRFi of 84.2% [vs CAB high-risk, HR, 0.48 (95% CI, 0.28-0.82), P = 0.009].
Conclusions: Cost-effective CAB is a statistically robust prognostic and predictive tool for ten-year DM for postmenopausal women with HR+/HER2-, early breast cancer. CAB low-risk patients who received exemestane monotherapy had an excellent ten-year DRFi.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


