Self-Triage Use, Subsequent Healthcare Utilization, and Diagnoses: A Retrospective Study of Process and Clinical Outcomes Following Self-Triage and Self-Scheduling for Ear or Hearing Symptoms.
Frederick North, Teresa B Jensen, Robert J Stroebel, Elissa M Nelson, Brenda J Johnson, Matthew C Thompson, Jennifer L Pecina, Brian A Crum
{"title":"Self-Triage Use, Subsequent Healthcare Utilization, and Diagnoses: A Retrospective Study of Process and Clinical Outcomes Following Self-Triage and Self-Scheduling for Ear or Hearing Symptoms.","authors":"Frederick North, Teresa B Jensen, Robert J Stroebel, Elissa M Nelson, Brenda J Johnson, Matthew C Thompson, Jennifer L Pecina, Brian A Crum","doi":"10.1177/23333928231168121","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Self-triage is becoming more widespread, but little is known about the people who are using online self-triage tools and their outcomes. For self-triage researchers, there are significant barriers to capturing subsequent healthcare outcomes. Our integrated healthcare system was able to capture subsequent healthcare utilization of individuals who used self-triage integrated with self-scheduling of provider visits.</p><p><strong>Methods: </strong>We retrospectively examined healthcare utilization and diagnoses after patients had used self-triage and self-scheduling for ear or hearing symptoms. Outcomes and counts of office visits, telemedicine interactions, emergency department visits, and hospitalizations were captured. Diagnosis codes associated with subsequent provider visits were dichotomously categorized as being associated with ear or hearing concerns or not. Nonvisit care encounters of patient-initiated messages, nurse triage calls, and clinical communications were also captured.</p><p><strong>Results: </strong>For 2168 self-triage uses, we were able to capture subsequent healthcare encounters within 7 days of the self-triage for 80.5% (1745/2168). In subsequent 1092 office visits with diagnoses, 83.1% (891/1092) of the uses were associated with relevant ear, nose and throat diagnoses. Only 0.24% (4/1662) of patients with captured outcomes were associated with a hospitalization within 7 days. Self-triage resulted in a self-scheduled office visit in 7.2% (126/1745). Office visits resulting from a self-scheduled visit had significantly fewer combined non-visit care encounters per office visit (fewer combined nurse triage calls, patient messages, and clinical communication messages) than office visits that were not self-scheduled (-0.51; 95% CI, -0.72 to -0.29; <i>P</i> < .0001).</p><p><strong>Conclusion: </strong>In an appropriate healthcare setting, self-triage outcomes can be captured in a high percentage of uses to examine for safety, patient adherence to recommendations, and efficiency of self-triage. With the ear or hearing self-triage, most uses had subsequent visit diagnoses relevant to ear or hearing, so most patients appeared to be selecting the appropriate self-triage pathway for their symptoms.</p>","PeriodicalId":12951,"journal":{"name":"Health Services Research and Managerial Epidemiology","volume":"10 ","pages":"23333928231168121"},"PeriodicalIF":1.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/50/a9/10.1177_23333928231168121.PMC10123887.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Research and Managerial Epidemiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23333928231168121","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Self-triage is becoming more widespread, but little is known about the people who are using online self-triage tools and their outcomes. For self-triage researchers, there are significant barriers to capturing subsequent healthcare outcomes. Our integrated healthcare system was able to capture subsequent healthcare utilization of individuals who used self-triage integrated with self-scheduling of provider visits.
Methods: We retrospectively examined healthcare utilization and diagnoses after patients had used self-triage and self-scheduling for ear or hearing symptoms. Outcomes and counts of office visits, telemedicine interactions, emergency department visits, and hospitalizations were captured. Diagnosis codes associated with subsequent provider visits were dichotomously categorized as being associated with ear or hearing concerns or not. Nonvisit care encounters of patient-initiated messages, nurse triage calls, and clinical communications were also captured.
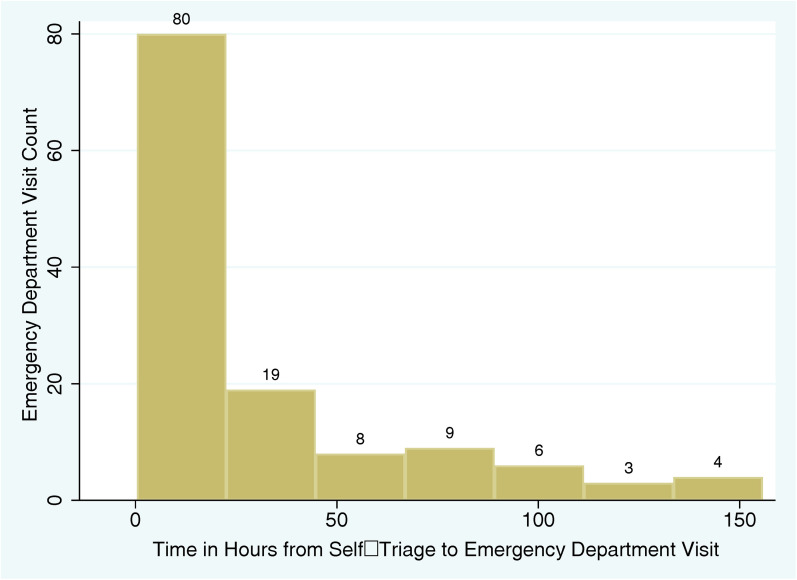
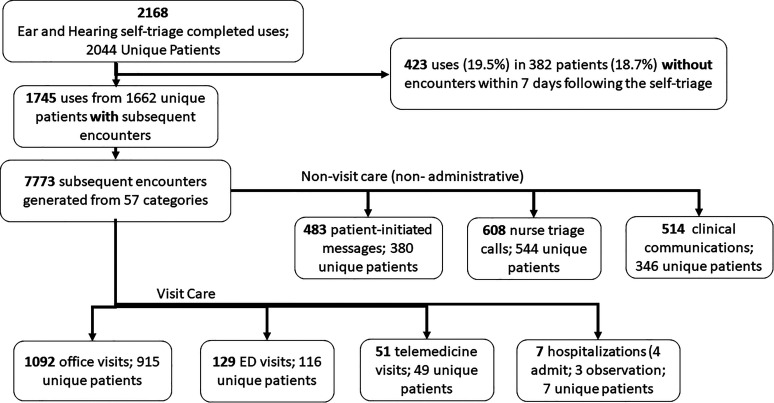
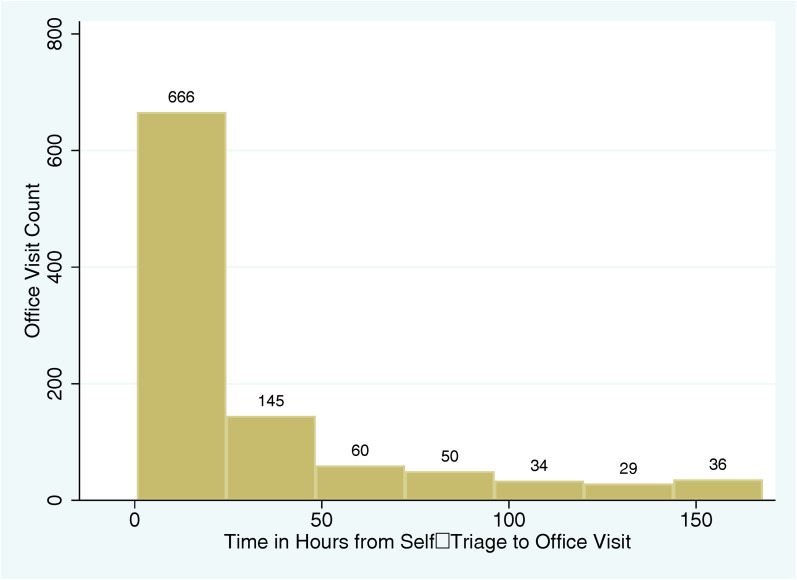
Results: For 2168 self-triage uses, we were able to capture subsequent healthcare encounters within 7 days of the self-triage for 80.5% (1745/2168). In subsequent 1092 office visits with diagnoses, 83.1% (891/1092) of the uses were associated with relevant ear, nose and throat diagnoses. Only 0.24% (4/1662) of patients with captured outcomes were associated with a hospitalization within 7 days. Self-triage resulted in a self-scheduled office visit in 7.2% (126/1745). Office visits resulting from a self-scheduled visit had significantly fewer combined non-visit care encounters per office visit (fewer combined nurse triage calls, patient messages, and clinical communication messages) than office visits that were not self-scheduled (-0.51; 95% CI, -0.72 to -0.29; P < .0001).
Conclusion: In an appropriate healthcare setting, self-triage outcomes can be captured in a high percentage of uses to examine for safety, patient adherence to recommendations, and efficiency of self-triage. With the ear or hearing self-triage, most uses had subsequent visit diagnoses relevant to ear or hearing, so most patients appeared to be selecting the appropriate self-triage pathway for their symptoms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


