{"title":"Safety of Left Subclavian Artery Selective Coverage without Revascularization in Thoracic Endovascular Aortic Repair for Type B Aortic Dissections.","authors":"Mingyu Sun, Yasong Wang, Tienan Zhou, Xuanze Liu, Quanmin Jing, Haiwei Liu, Xiaozeng Wang","doi":"10.5761/atcs.oa.22-00146","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Whether to proceed left subclavian artery (LSA) revascularization in patients with LSA coverage due to insufficient proximal landing zone (PLZ) during thoracic endovascular aortic repair (TEVAR) remains controversial.</p><p><strong>Methods: </strong>A total of 903 patients who received TEVAR were retrospectively analyzed. LSA could be covered if the PLZ was less than 15 mm accompanied with 1) a dominant or balanced right vertebral artery, 2) a complete circle of Willis, and 3) a left vertebral artery with a diameter ≥3 mm and without severe stenosis.</p><p><strong>Results: </strong>LSA selective coverage was necessary for 35.0% (316/903) of the patients to extend the PLZ. Patients presented with weakness, pain, cooling and discoloration of the left upper extremity (LUE), and pulselessness of the left brachial artery were more in the LSA-covered group. The ischemia of LUE occurred more often in patients with LSA covered completely than in those with LSA covered partially. Functional arm status showed no significant difference in the arm, shoulder, and hand questionnaire scores at 12 months postoperative between the LSA-covered group and LSA-uncovered group, or between the LSA-covered completely group and LSA-covered partially group.</p><p><strong>Conclusion: </strong>It was safe to cover the LSA origin without revascularization if the PLZ was less than 15 mm accompanied with careful evaluation (description in method).</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"29 2","pages":"70-77"},"PeriodicalIF":1.3000,"publicationDate":"2023-04-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4e/ca/atcs-29-070.PMC10126769.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.22-00146","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: Whether to proceed left subclavian artery (LSA) revascularization in patients with LSA coverage due to insufficient proximal landing zone (PLZ) during thoracic endovascular aortic repair (TEVAR) remains controversial.
Methods: A total of 903 patients who received TEVAR were retrospectively analyzed. LSA could be covered if the PLZ was less than 15 mm accompanied with 1) a dominant or balanced right vertebral artery, 2) a complete circle of Willis, and 3) a left vertebral artery with a diameter ≥3 mm and without severe stenosis.
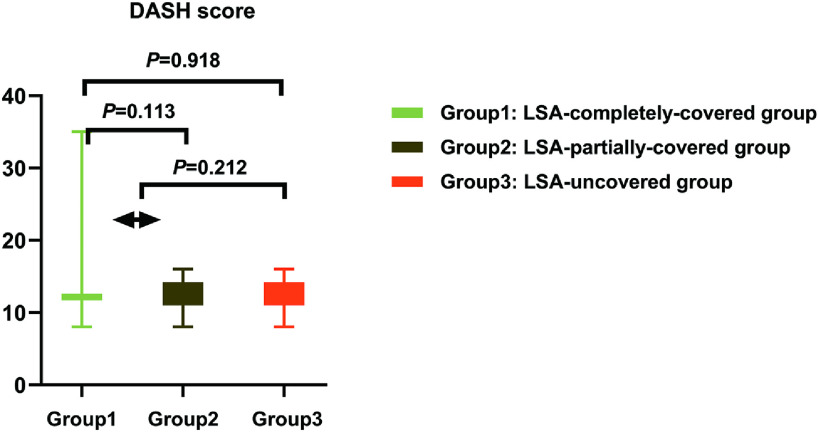
Results: LSA selective coverage was necessary for 35.0% (316/903) of the patients to extend the PLZ. Patients presented with weakness, pain, cooling and discoloration of the left upper extremity (LUE), and pulselessness of the left brachial artery were more in the LSA-covered group. The ischemia of LUE occurred more often in patients with LSA covered completely than in those with LSA covered partially. Functional arm status showed no significant difference in the arm, shoulder, and hand questionnaire scores at 12 months postoperative between the LSA-covered group and LSA-uncovered group, or between the LSA-covered completely group and LSA-covered partially group.
Conclusion: It was safe to cover the LSA origin without revascularization if the PLZ was less than 15 mm accompanied with careful evaluation (description in method).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


