{"title":"Factors that influence clinical decisions about offering parent coaching for autistic youth served within the Medicaid system.","authors":"Diondra Straiton, Kyle Frost, Brooke Ingersoll","doi":"10.1177/26334895231153631","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Parent coaching is an evidence-based practice for young autistic children, but it is underutilized in lower-resourced community settings like the Medicaid system (Straiton et al., 2021b). Clinicians often struggle to implement parent coaching with low-income and marginalized families (Tomczuk et al., 2022), but little is known about which factors influence clinician decision making processes about providing parent coaching to this population.</p><p><strong>Methods: </strong>This qualitative analysis used the framework method and thematic analysis. We used the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework (Aarons et al., 2011) to identify factors in the clinical decision-making process that community providers use when offering parent coaching to families of Medicaid-enrolled autistic children. Interviews with 13 providers and a focus group with 13 providers were analyzed.</p><p><strong>Results: </strong>The following themes emerged: 1) Policies drive provider task priorities and affect competing demands; 2) Providers are more likely to use parent coaching when agency leaders monitor parent coaching benchmarks, though this is rarely done; 3) Logistical factors like scheduling and treatment location affect perceived feasibility of using parent coaching; 4) Previous experience or coursework in parent coaching and/or family systems supports the quality of parent coaching implementation; 5) Provider perceptions of \"parent readiness\" are initially indicated by overt expressions of parent interest.</p><p><strong>Conclusions: </strong>In the absence of outer-context and inner-context policies, providers have more decision-making power to offer parent coaching based on their own judgements and preferences, which may result in fewer families being offered parent coaching and increased bias related to which families are offered this service. State-, agency-, and clinician-level recommendations are provided for increasing equitable provision of this evidence-based practice for autism.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"4 ","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8d/f2/10.1177_26334895231153631.PMC9978664.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895231153631","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/2/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Parent coaching is an evidence-based practice for young autistic children, but it is underutilized in lower-resourced community settings like the Medicaid system (Straiton et al., 2021b). Clinicians often struggle to implement parent coaching with low-income and marginalized families (Tomczuk et al., 2022), but little is known about which factors influence clinician decision making processes about providing parent coaching to this population.
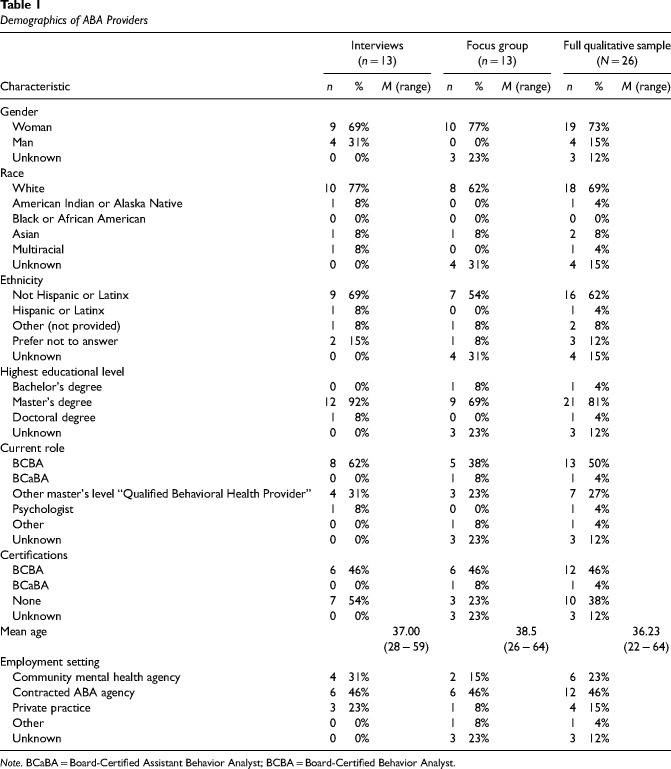
Methods: This qualitative analysis used the framework method and thematic analysis. We used the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework (Aarons et al., 2011) to identify factors in the clinical decision-making process that community providers use when offering parent coaching to families of Medicaid-enrolled autistic children. Interviews with 13 providers and a focus group with 13 providers were analyzed.
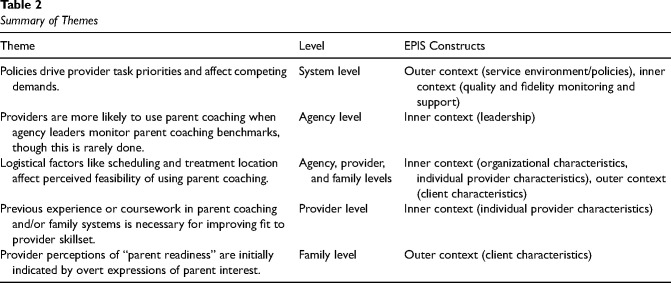
Results: The following themes emerged: 1) Policies drive provider task priorities and affect competing demands; 2) Providers are more likely to use parent coaching when agency leaders monitor parent coaching benchmarks, though this is rarely done; 3) Logistical factors like scheduling and treatment location affect perceived feasibility of using parent coaching; 4) Previous experience or coursework in parent coaching and/or family systems supports the quality of parent coaching implementation; 5) Provider perceptions of "parent readiness" are initially indicated by overt expressions of parent interest.
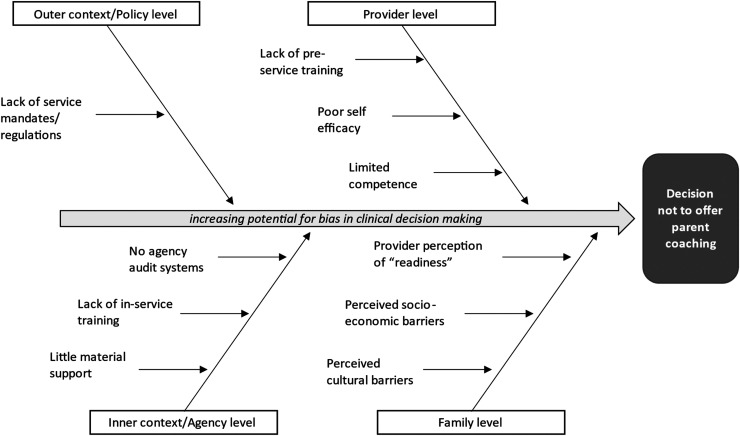
Conclusions: In the absence of outer-context and inner-context policies, providers have more decision-making power to offer parent coaching based on their own judgements and preferences, which may result in fewer families being offered parent coaching and increased bias related to which families are offered this service. State-, agency-, and clinician-level recommendations are provided for increasing equitable provision of this evidence-based practice for autism.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


