Kimberly D Williams, Beverly L Wilson, Claudine T Jurkovitz, Jo A Melson, Jeffrey A Reitz, Carmen K Pal, Sherry P Hausman, Erin Booker, Linda J Lang, Terry L Horton
{"title":"Implementation of a clinical pathway to screen and treat medical inpatients for opioid withdrawal.","authors":"Kimberly D Williams, Beverly L Wilson, Claudine T Jurkovitz, Jo A Melson, Jeffrey A Reitz, Carmen K Pal, Sherry P Hausman, Erin Booker, Linda J Lang, Terry L Horton","doi":"10.1177/26334895221096290","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Opioid-related inpatient hospital stays are increasing at alarming rates. Unidentified and poorly treated opioid withdrawal may be associated with inpatients leaving against medical advice and increased health care utilization. To address these concerns, we developed and implemented a clinical pathway to screen and treat medical service inpatients for opioid withdrawal.</p><p><strong>Methods: </strong>The pathway process included a two-item universal screening instrument to identify opioid withdrawal risk (Opioid Withdrawal Risk Assessment [OWRA]), use of the validated Clinical Opiate Withdrawal Scale (COWS) to monitor opioid withdrawal symptoms and severity, and a 72-h buprenorphine/naloxone-based treatment protocol. Implementation outcomes including adoption, fidelity, and sustainability of this new pathway model were measured. To assess if there were changes in nursing staff acceptability, appropriateness, and adoption of the new pathway process, a cross-sectional survey was administered to pilot four hospital medical units before and after pathway implementation.</p><p><strong>Results: </strong>Between 2016 and 2018, 72.4% (77,483/107,071) of admitted patients received the OWRA screening tool. Of those, 3.0% (2,347/77,483) were identified at risk for opioid withdrawal. Of those 2,347 patients, 2,178 (92.8%) were assessed with the COWS and 29.6% (645/2,178) were found to be in active withdrawal. A total of 49.5% (319/645) patients were treated with buprenorphine/naloxone. Fifty-seven percent (83/145) of nurses completed both the pre- and post-pathway implementation surveys. Analysis of the pre/post survey data revealed that nurse respondents were more confident in their ability to determine which patients were at risk for withdrawal (<i>p</i> = .01) and identify patients currently experiencing withdrawal (<i>p</i> < .01). However, they cited difficulty working with the patient population and coordinating care with physicians.</p><p><strong>Conclusions: </strong>Our study demonstrates a process for successfully implementing and sustaining a clinical pathway to screen and treat medical service inpatients for opioid withdrawal. Standardizing care delivery for patients in opioid withdrawal can also improve nursing confidence when working with this complex population.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"3 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/19/40/10.1177_26334895221096290.PMC9281054.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895221096290","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/4/27 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Opioid-related inpatient hospital stays are increasing at alarming rates. Unidentified and poorly treated opioid withdrawal may be associated with inpatients leaving against medical advice and increased health care utilization. To address these concerns, we developed and implemented a clinical pathway to screen and treat medical service inpatients for opioid withdrawal.
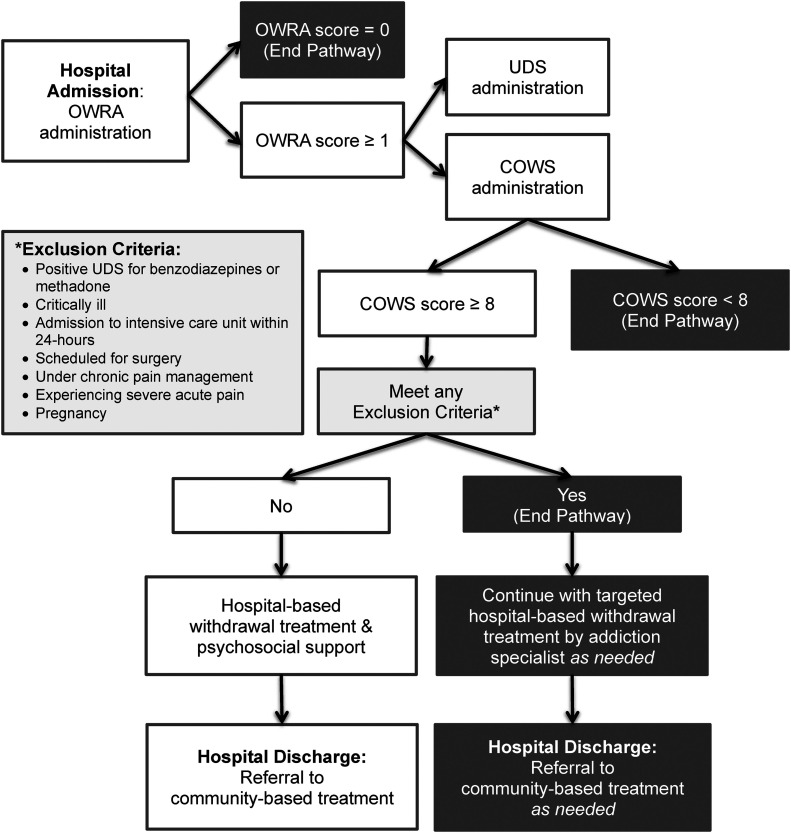
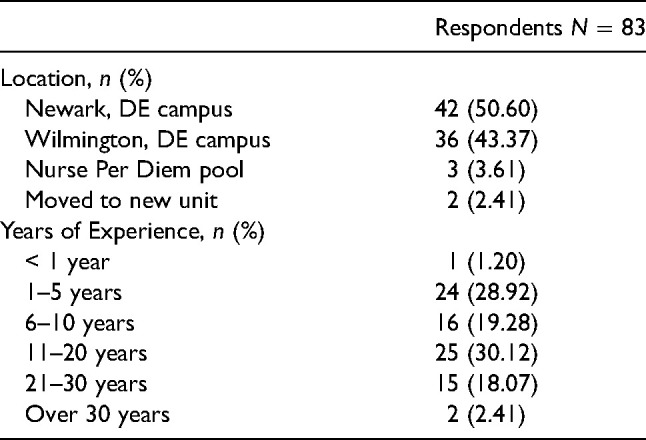
Methods: The pathway process included a two-item universal screening instrument to identify opioid withdrawal risk (Opioid Withdrawal Risk Assessment [OWRA]), use of the validated Clinical Opiate Withdrawal Scale (COWS) to monitor opioid withdrawal symptoms and severity, and a 72-h buprenorphine/naloxone-based treatment protocol. Implementation outcomes including adoption, fidelity, and sustainability of this new pathway model were measured. To assess if there were changes in nursing staff acceptability, appropriateness, and adoption of the new pathway process, a cross-sectional survey was administered to pilot four hospital medical units before and after pathway implementation.
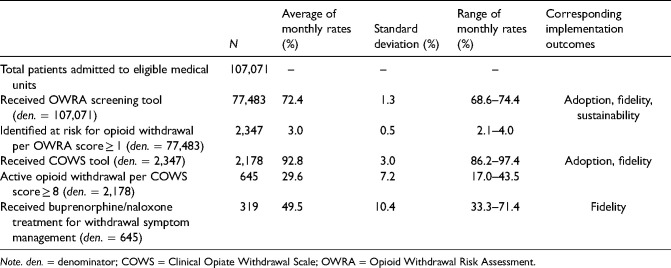
Results: Between 2016 and 2018, 72.4% (77,483/107,071) of admitted patients received the OWRA screening tool. Of those, 3.0% (2,347/77,483) were identified at risk for opioid withdrawal. Of those 2,347 patients, 2,178 (92.8%) were assessed with the COWS and 29.6% (645/2,178) were found to be in active withdrawal. A total of 49.5% (319/645) patients were treated with buprenorphine/naloxone. Fifty-seven percent (83/145) of nurses completed both the pre- and post-pathway implementation surveys. Analysis of the pre/post survey data revealed that nurse respondents were more confident in their ability to determine which patients were at risk for withdrawal (p = .01) and identify patients currently experiencing withdrawal (p < .01). However, they cited difficulty working with the patient population and coordinating care with physicians.
Conclusions: Our study demonstrates a process for successfully implementing and sustaining a clinical pathway to screen and treat medical service inpatients for opioid withdrawal. Standardizing care delivery for patients in opioid withdrawal can also improve nursing confidence when working with this complex population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


