Shelley Ohliger, Alain Harb, Caroline Al-Haddadin, David P Bennett, Tiffany Frazee, Cassandra Hoffmann
{"title":"Addition of Deep Parasternal Plane Block to Enhanced Recovery Protocol for Pediatric Cardiac Surgery.","authors":"Shelley Ohliger, Alain Harb, Caroline Al-Haddadin, David P Bennett, Tiffany Frazee, Cassandra Hoffmann","doi":"10.2147/LRA.S387631","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aims to evaluate if the addition of deep parasternal plane blocks to a pre-existing enhanced recovery pathway for pediatric cardiac surgery improves outcomes.</p><p><strong>Patients and methods: </strong>A retrospective review through an EMR query from June 2019 to June 2021 was performed for patients less than 18 years of age who underwent cardiac surgery via median sternotomy and were extubated immediately following surgery in a single academic tertiary care hospital. Patients receiving deep parasternal blocks as part of an enhanced recovery protocol were compared to similar patients from the year prior to block implementation.</p><p><strong>Results: </strong>The primary outcome was intraoperative and postoperative opioid consumption. Secondary outcomes were pain scores, intensive care unit (ICU) length of stay and time to first oral intake. There was a statistically significant reduction in intraoperative opioid administration and pain scores in the first 24 hours post-operatively. There was also a statistically significant reduction in ICU length of stay. There was no statistically significant difference in post-operative opioid consumption and time to first oral intake.</p><p><strong>Conclusion: </strong>Bilateral deep parasternal blocks may reduce opioid consumption, provide effective postoperative pain control, and result in decreased length of intensive care unit stay across both simple and complex pediatric cardiac procedures when added to a pre-existing enhanced recovery protocol.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"16 ","pages":"11-18"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0c/18/lra-16-11.PMC9940490.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S387631","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study aims to evaluate if the addition of deep parasternal plane blocks to a pre-existing enhanced recovery pathway for pediatric cardiac surgery improves outcomes.
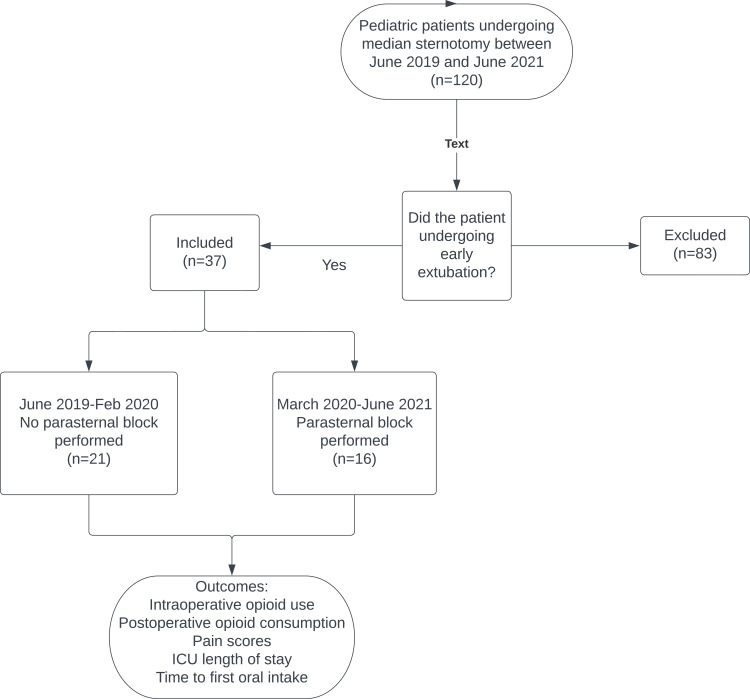
Patients and methods: A retrospective review through an EMR query from June 2019 to June 2021 was performed for patients less than 18 years of age who underwent cardiac surgery via median sternotomy and were extubated immediately following surgery in a single academic tertiary care hospital. Patients receiving deep parasternal blocks as part of an enhanced recovery protocol were compared to similar patients from the year prior to block implementation.
Results: The primary outcome was intraoperative and postoperative opioid consumption. Secondary outcomes were pain scores, intensive care unit (ICU) length of stay and time to first oral intake. There was a statistically significant reduction in intraoperative opioid administration and pain scores in the first 24 hours post-operatively. There was also a statistically significant reduction in ICU length of stay. There was no statistically significant difference in post-operative opioid consumption and time to first oral intake.
Conclusion: Bilateral deep parasternal blocks may reduce opioid consumption, provide effective postoperative pain control, and result in decreased length of intensive care unit stay across both simple and complex pediatric cardiac procedures when added to a pre-existing enhanced recovery protocol.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


