Muhammad U Manzoor, Abdullah A Alrashed, Ibrahim A Almulhim, Sultan Alqahtani, Fahmi Al Senani
{"title":"Ulnar artery access for intracranial mechanical thrombectomy procedure: A salvage option after failed trans-femoral and trans-radial access.","authors":"Muhammad U Manzoor, Abdullah A Alrashed, Ibrahim A Almulhim, Sultan Alqahtani, Fahmi Al Senani","doi":"10.7461/jcen.2023.E2022.10.012","DOIUrl":null,"url":null,"abstract":"<p><p>84 years old gentle man with past medical history of hypertension and diabetes presented with sudden onset right sided weakness and aphasia for two hours. Initial neurological assessment revealed National Institute of Health Stroke Scale (NIHSS) 17. Computed tomography (CT) scan demonstrated minimal early ischemic changes along left insular cortex with occlusion of left middle cerebral artery (MCA). Based on clinical and imaging findings, decision was made to perform mechanical thrombectomy procedure. Initially, right common femoral artery approach was utilized. However, due to unfavorable type-III bovine arch, left internal carotid artery could not be engaged via this approach. Subsequently, access was switched to right radial artery. Angiogram revealed small caliber radial artery, with larger caliber ulnar artery. Attempt was made to advance the guide catheter through the radial artery, however significant vasospasm was encountered. Subsequently, ulnar artery was accessed and successful thrombolysis in cerebral infarction (TICI) III left MCA reperfusion was achieved with a single pass of mechanical thrombectomy via this approach. Post procedure neurological examination demonstrated significant clinical improvement. Doppler ultrasound 48 hours after the procedure demonstrated patent flow in radial and ulnar arteries with no evidence of dissection.</p>","PeriodicalId":15359,"journal":{"name":"Journal of Cerebrovascular and Endovascular Neurosurgery","volume":" ","pages":"429-433"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10774676/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cerebrovascular and Endovascular Neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7461/jcen.2023.E2022.10.012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/2/20 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
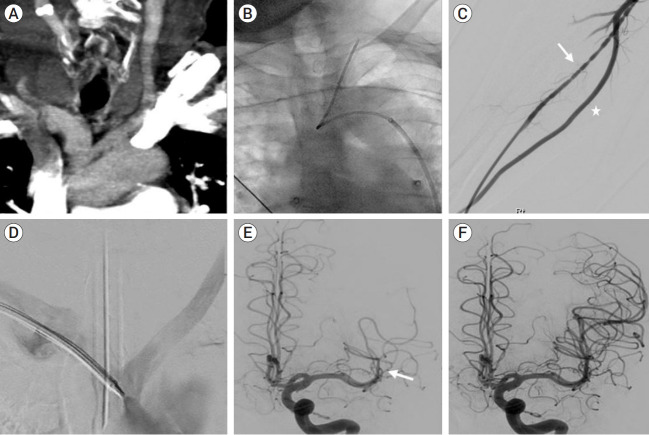
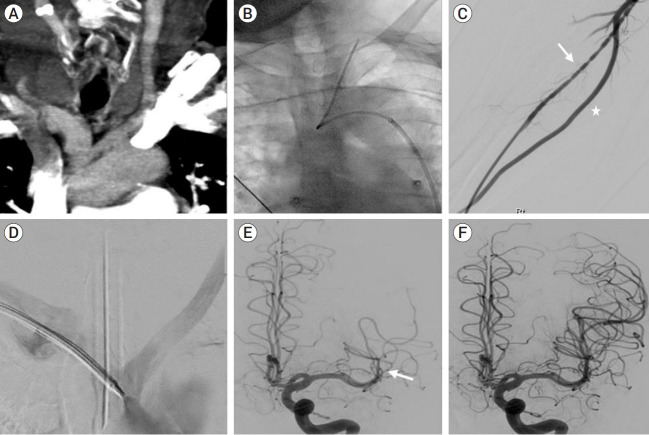
84 years old gentle man with past medical history of hypertension and diabetes presented with sudden onset right sided weakness and aphasia for two hours. Initial neurological assessment revealed National Institute of Health Stroke Scale (NIHSS) 17. Computed tomography (CT) scan demonstrated minimal early ischemic changes along left insular cortex with occlusion of left middle cerebral artery (MCA). Based on clinical and imaging findings, decision was made to perform mechanical thrombectomy procedure. Initially, right common femoral artery approach was utilized. However, due to unfavorable type-III bovine arch, left internal carotid artery could not be engaged via this approach. Subsequently, access was switched to right radial artery. Angiogram revealed small caliber radial artery, with larger caliber ulnar artery. Attempt was made to advance the guide catheter through the radial artery, however significant vasospasm was encountered. Subsequently, ulnar artery was accessed and successful thrombolysis in cerebral infarction (TICI) III left MCA reperfusion was achieved with a single pass of mechanical thrombectomy via this approach. Post procedure neurological examination demonstrated significant clinical improvement. Doppler ultrasound 48 hours after the procedure demonstrated patent flow in radial and ulnar arteries with no evidence of dissection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


