{"title":"Prognostic Predictors of Tricuspid Regurgitation Worsening after Mitral Regurgitation Surgery with Mild Tricuspid Regurgitation","authors":"","doi":"10.1053/j.semtcvs.2023.03.003","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>We aimed to investigate the prevalence and predictors of postoperative tricuspid regurgitation (TR) worsening in patients with </span>mitral regurgitation<span> (MR) and concomitant ≤mild TR. A total of 620 patients underwent surgery for MR from 2013 to 2017. Of these, 260 had ≤mild preoperative TR and no concomitant tricuspid valve surgery and were enrolled in this single-center retrospective study. The primary endpoint was postoperative worsening of ≥moderate TR. The primary endpoint occurred in 28 of 260 patients (11%) during the follow-up period [median: 4.1 years (interquartile range: 2.9−6.1 years)]. In the multivariable analysis, age, female sex, and left atrial volume index (LAVI) were significant predictors of the primary outcome during intermediate-term follow-up (age: hazard ratio [HR] 1.05 per 1-year increment, 95% confidence interval [CI] 1.02–1.10, </span></span><em>P</em> = 0.003; female sex: HR 3.53, 95% CI 1.61–7.72, <em>P</em> = 0.002; LAVI: HR 1.17 per 10-mL/m<sup>2</sup> increment, 95% CI 1.07−1.26, <em>P</em> < 0.001). The optimal LAVI cut-off value for predicting postoperative TR worsening was 79 mL/m<sup>2</sup> (area under the curve: 0.69). A high LAVI (>79 mL/m²) was significantly associated with a low rate of freedom from postoperative TR worsening compared with a low LAVI (≤79 mL/m²) (82.6% vs 93.9% at 5 years, respectively; log-rank <em>P</em><span> = 0.008). In patients with ≤mild preoperative TR and no concomitant tricuspid surgery, the rate of postoperative TR worsening was 11% during intermediate-term follow-up. LA enlargement in patients with MR and ≤mild preoperative TR was significantly associated with postoperative TR worsening.</span></p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 3","pages":"Pages 303-312"},"PeriodicalIF":2.6000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067923000424","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
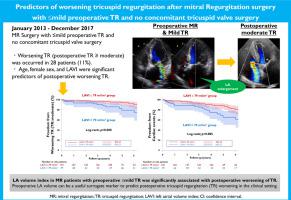
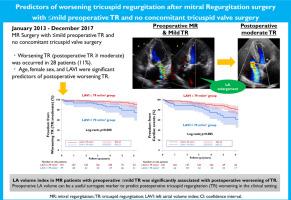
We aimed to investigate the prevalence and predictors of postoperative tricuspid regurgitation (TR) worsening in patients with mitral regurgitation (MR) and concomitant ≤mild TR. A total of 620 patients underwent surgery for MR from 2013 to 2017. Of these, 260 had ≤mild preoperative TR and no concomitant tricuspid valve surgery and were enrolled in this single-center retrospective study. The primary endpoint was postoperative worsening of ≥moderate TR. The primary endpoint occurred in 28 of 260 patients (11%) during the follow-up period [median: 4.1 years (interquartile range: 2.9−6.1 years)]. In the multivariable analysis, age, female sex, and left atrial volume index (LAVI) were significant predictors of the primary outcome during intermediate-term follow-up (age: hazard ratio [HR] 1.05 per 1-year increment, 95% confidence interval [CI] 1.02–1.10, P = 0.003; female sex: HR 3.53, 95% CI 1.61–7.72, P = 0.002; LAVI: HR 1.17 per 10-mL/m2 increment, 95% CI 1.07−1.26, P < 0.001). The optimal LAVI cut-off value for predicting postoperative TR worsening was 79 mL/m2 (area under the curve: 0.69). A high LAVI (>79 mL/m²) was significantly associated with a low rate of freedom from postoperative TR worsening compared with a low LAVI (≤79 mL/m²) (82.6% vs 93.9% at 5 years, respectively; log-rank P = 0.008). In patients with ≤mild preoperative TR and no concomitant tricuspid surgery, the rate of postoperative TR worsening was 11% during intermediate-term follow-up. LA enlargement in patients with MR and ≤mild preoperative TR was significantly associated with postoperative TR worsening.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


